
|
|
|
|
Avoid Incisive Canal
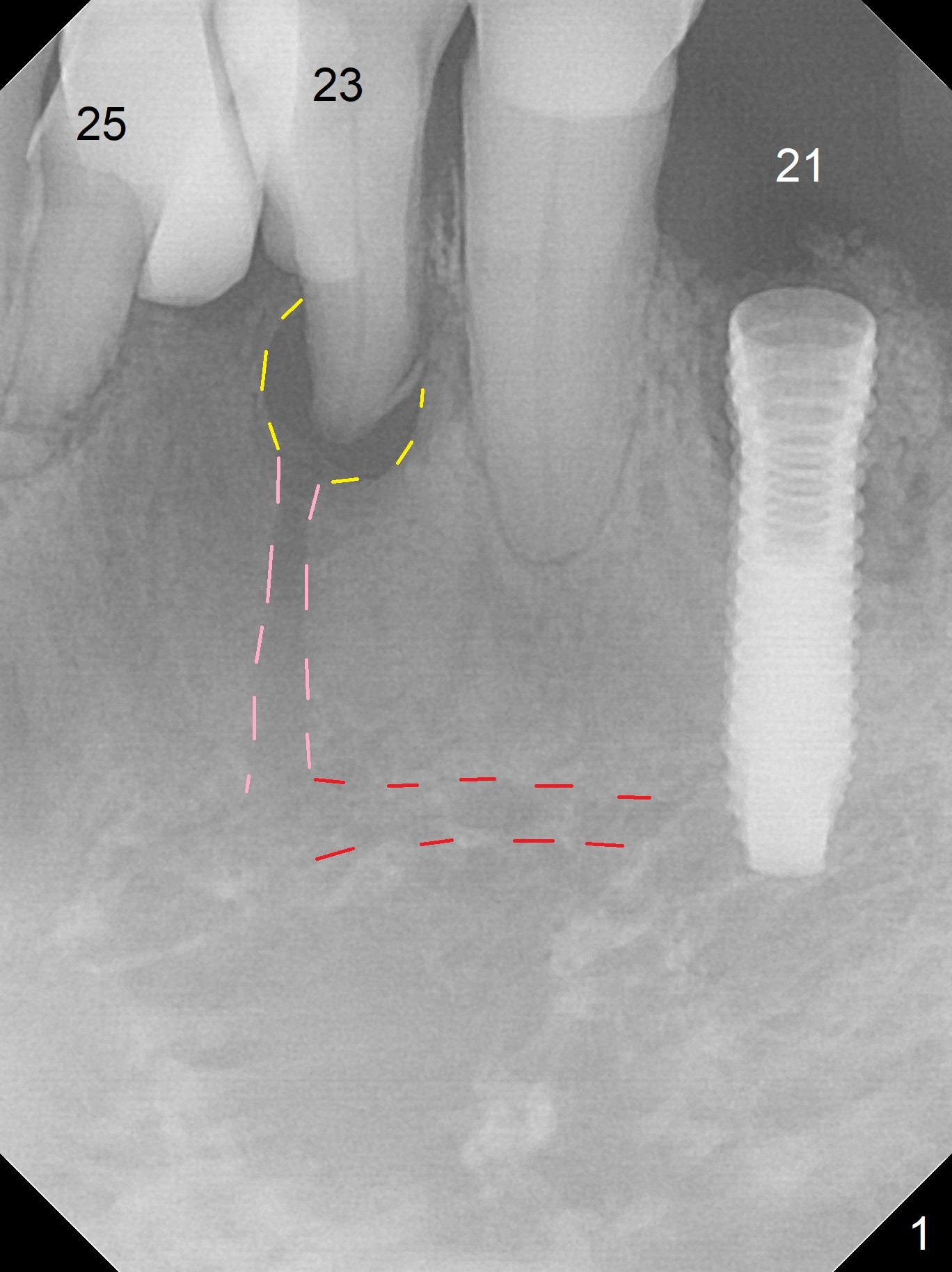
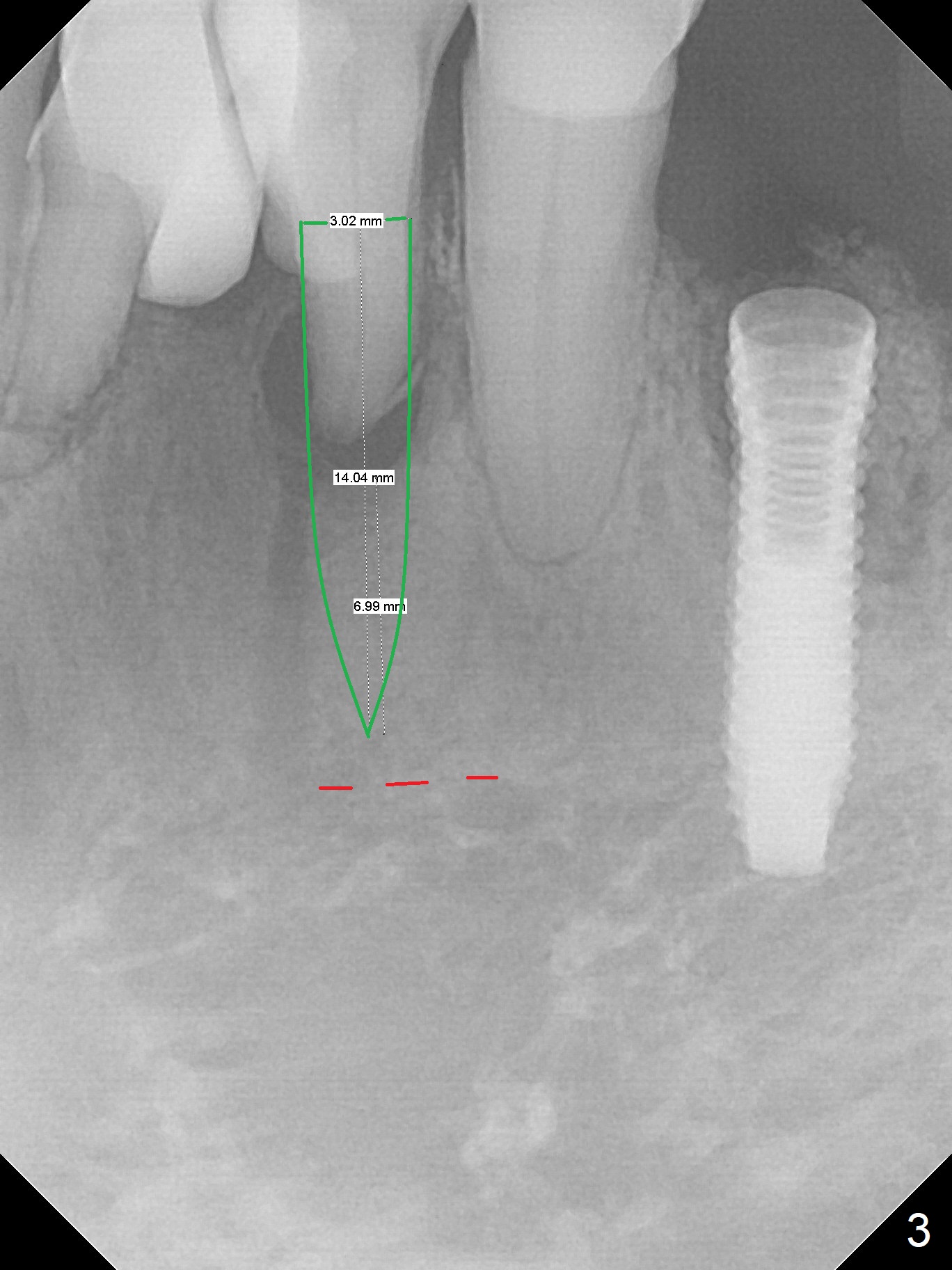
A 73-year-old man will return for #23 and 25 implants following ones at #21 and 31. Probably due to large periapical radiolucency at #23 (Fig.1 yellow dashed line), the terminal branch (pink) of the Incisive Canal (red) is distinct. Postop hemorrhage occurs associated with placement of a long implant at #. To prevent the complication at #23, a 14 mm long 1-piece implant (Fig.3) seems to be safer than 16 mm one (Fig.2). Seven mm in the native bone (Fig.3) should provide with sufficient primary stability. A temporary crown will be fabricated at #31. If the provisional at #21 is unstable, impression may be necessary for #21 and 31. Initiate osteotomy using visual and tactile acuity and double check the position and trajectory with RPD and X-ray. It might be preferable to extract the malpositioned incisor to give the remaining one the best 3-dimensional reference. Prepare 2 of 1-piece implant kits as well as angled one.
Return to
Lower Incisor Immediate Implant,
IBS,
No Antibiotic
Xin Wei, DDS, PhD, MS 1st edition 07/04/2017, last revision 06/02/2018