




|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|||
Immediate Repositioning of Implant
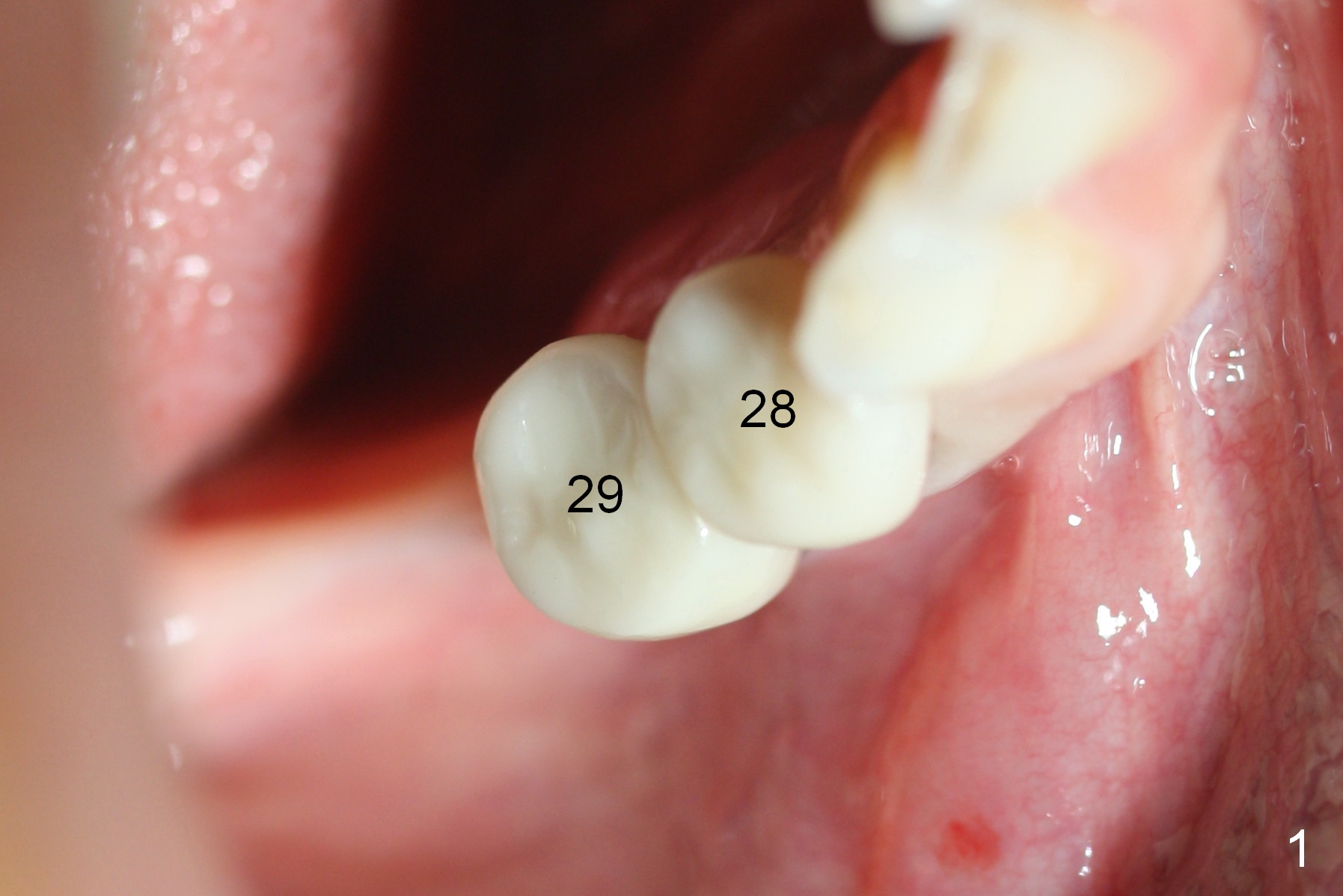
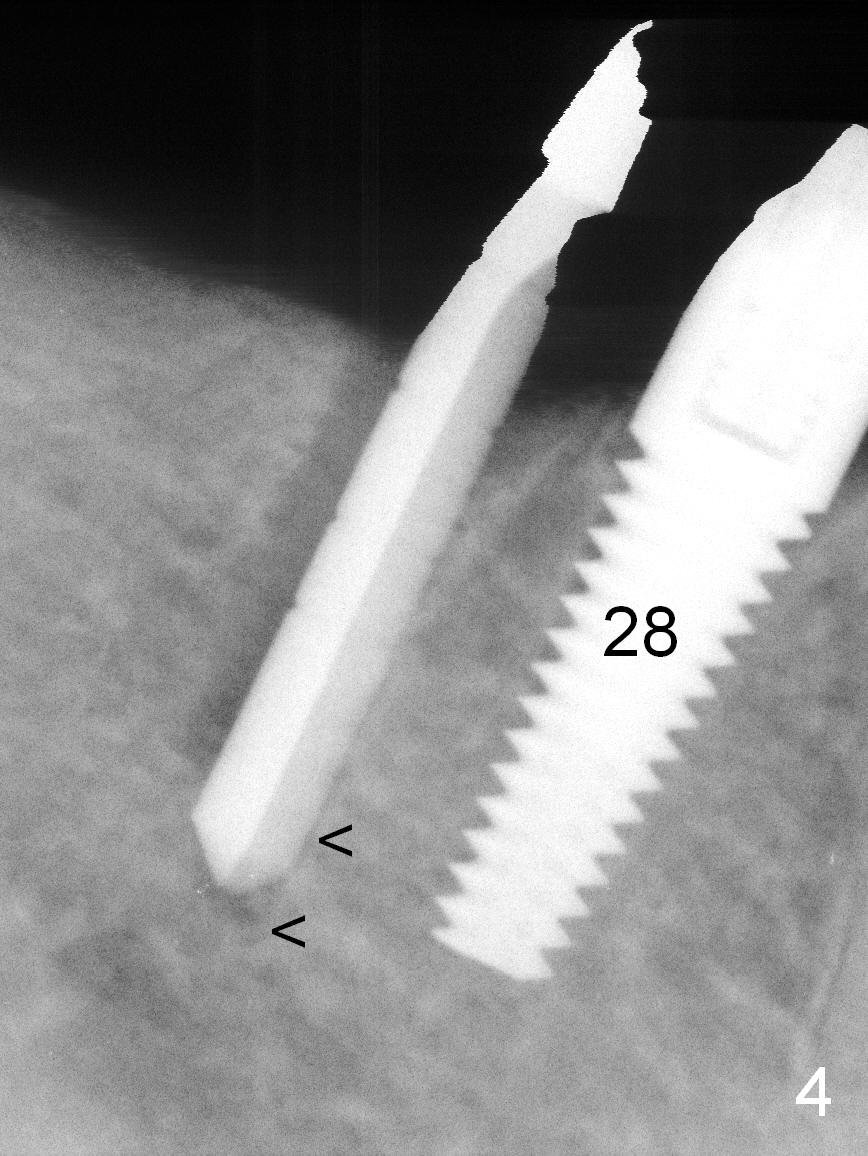
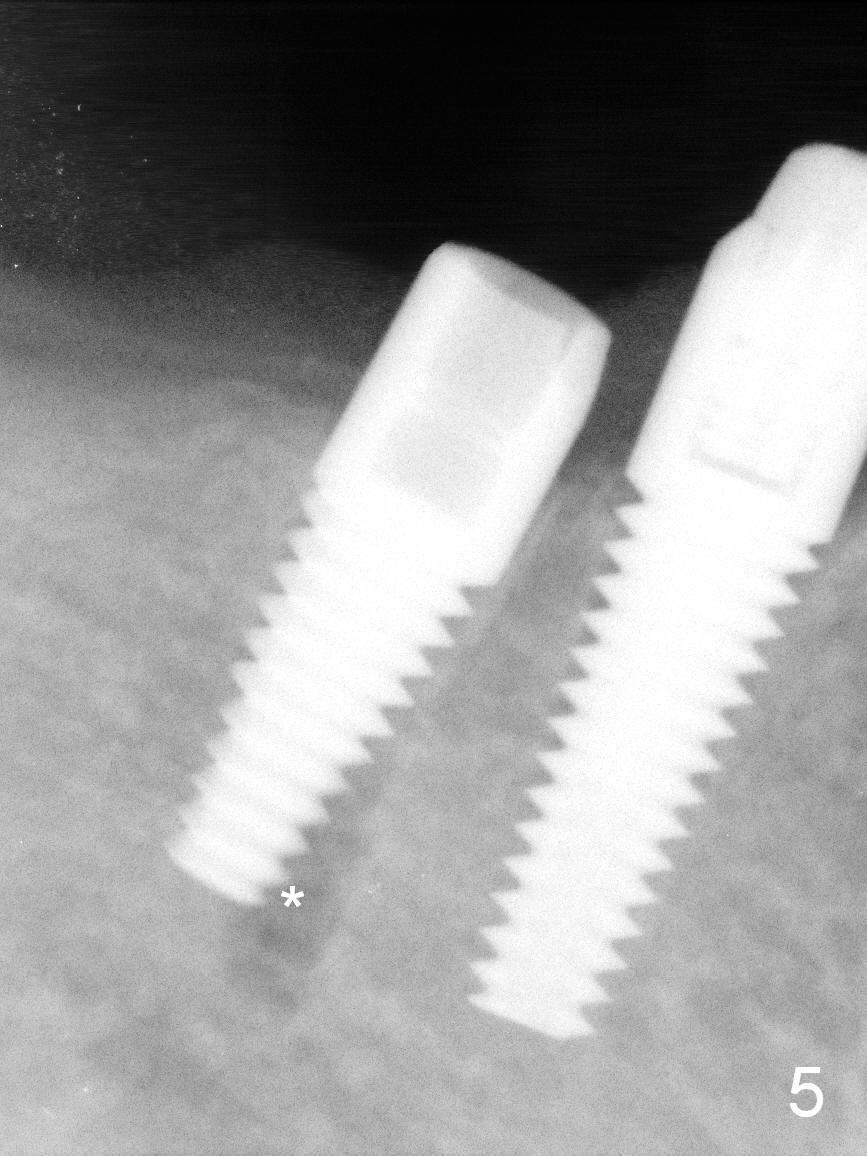
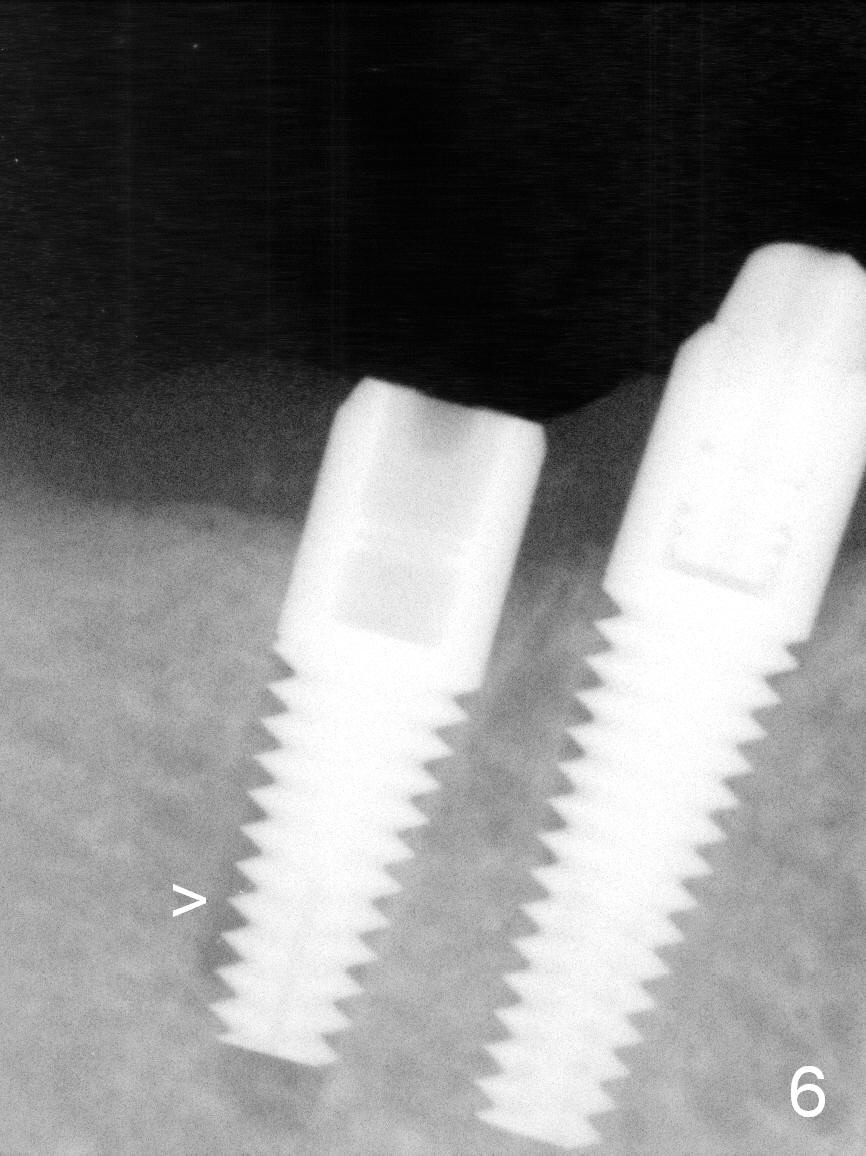
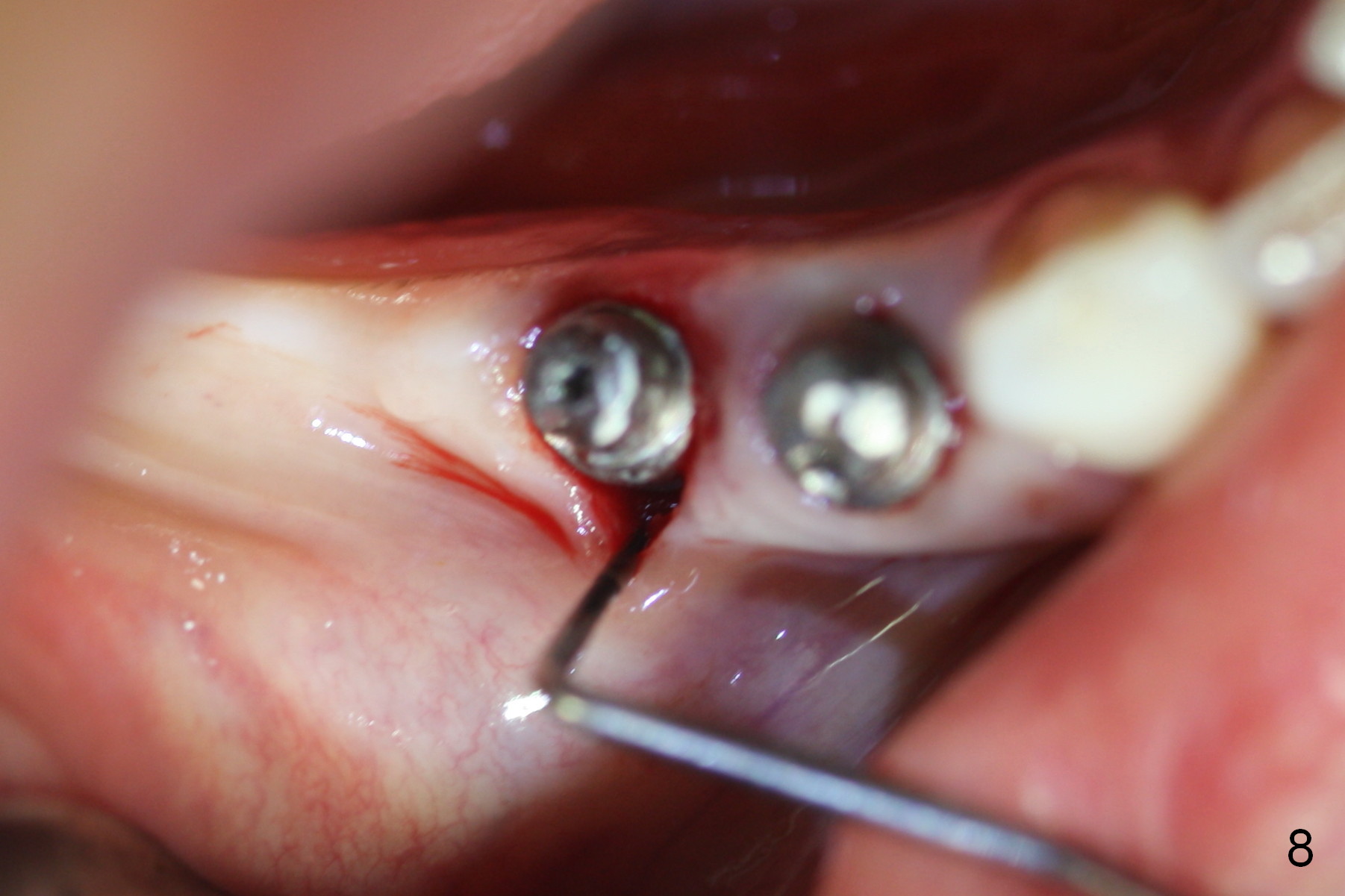
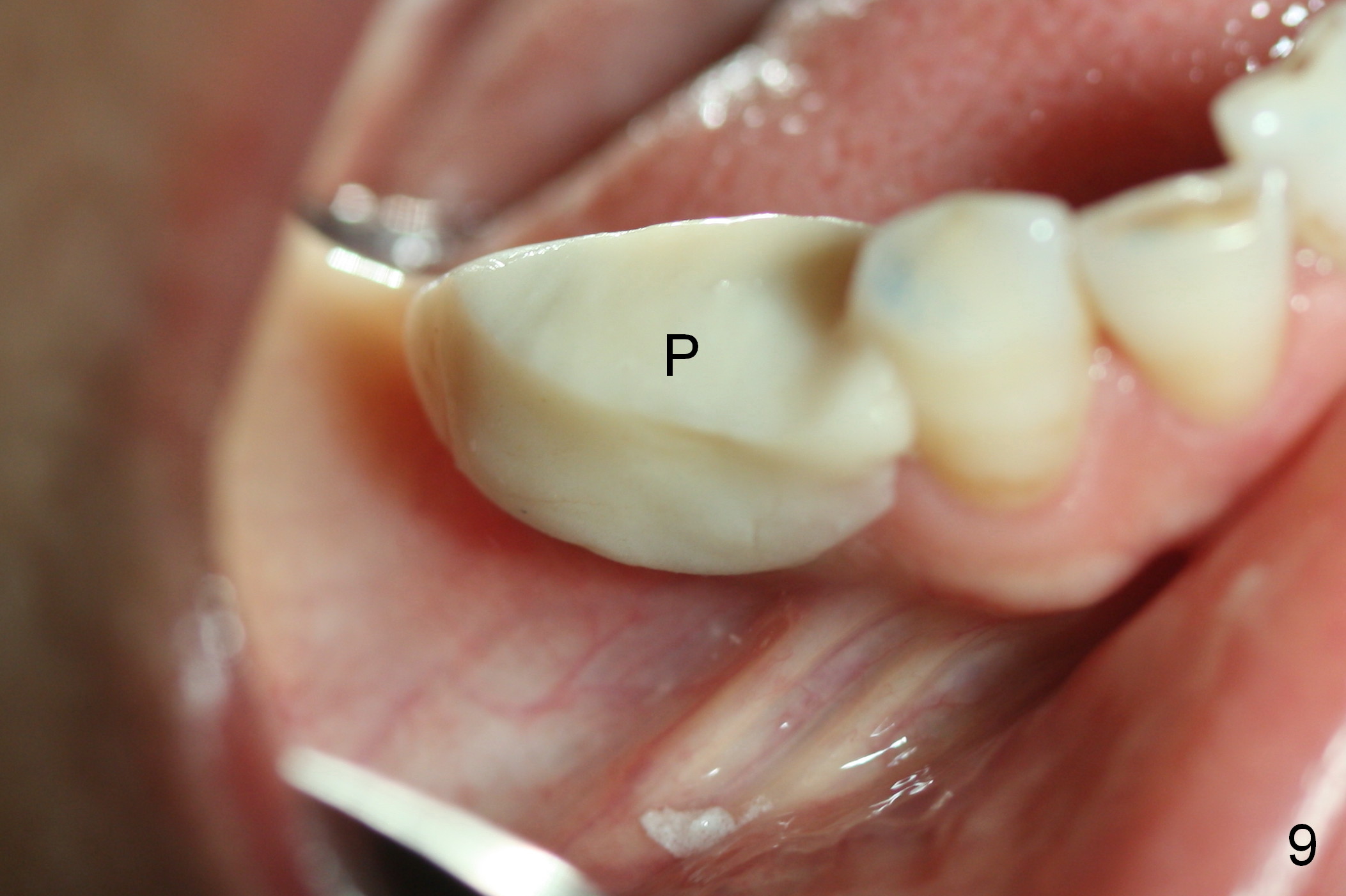
The patient complains of discomfort in mastication on the right. The position of the crowns at #28,29 seems to be normal (Fig.1). It is obvious that the implant/abutment at #29 is buccal (Fig.2 >) when the crown is removed. It remains so when the crown at #28 is removed (Fig.3). It is easy to un-torque the implant at #29. A Lindamann bur is used to remove ~ 2 mm of the lingual bone. A new osteotomy is initiated in the mesiolingual aspect (Fig.4 between arrowheads (<)). After osteotomy is finished with a 3.5x14 mm drill (underprep), the same implant is placed; it happens to be deviated from the new osteotomy (Fig.5 (*). After removal of the implant, the osteotomy is enlarged with a 4.0x14 mm drill and the implant is placed in a correct trajectory (Fig.6 (>: "old" osteotomy)) and position (Fig.7). The buccal gap is approximately 1 mm (Fig.8), where a small amount of autogenous bone is placed. A splinted provisional is fabricated at #28 and 29 to keep the graft in place (Fig.9 P).
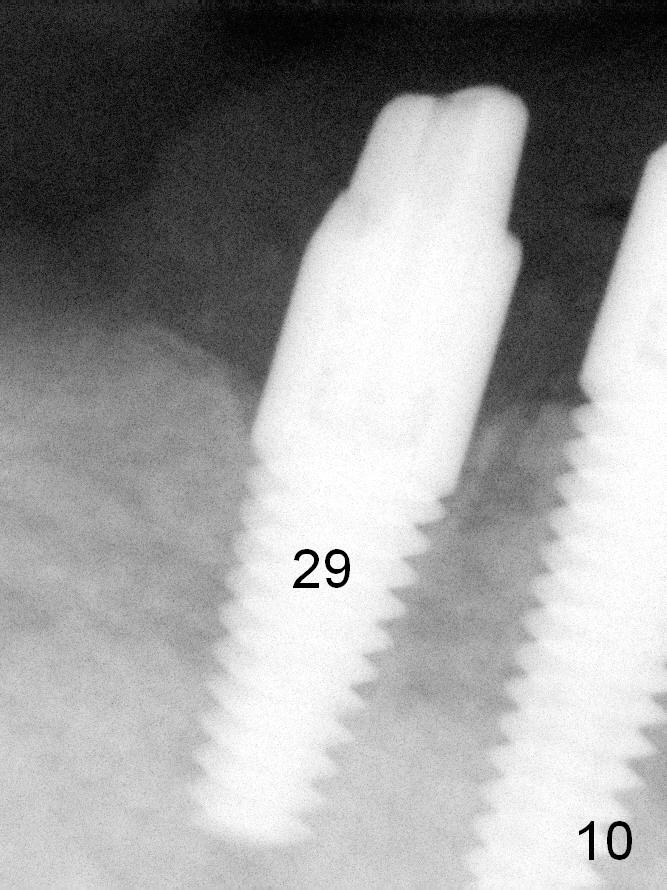
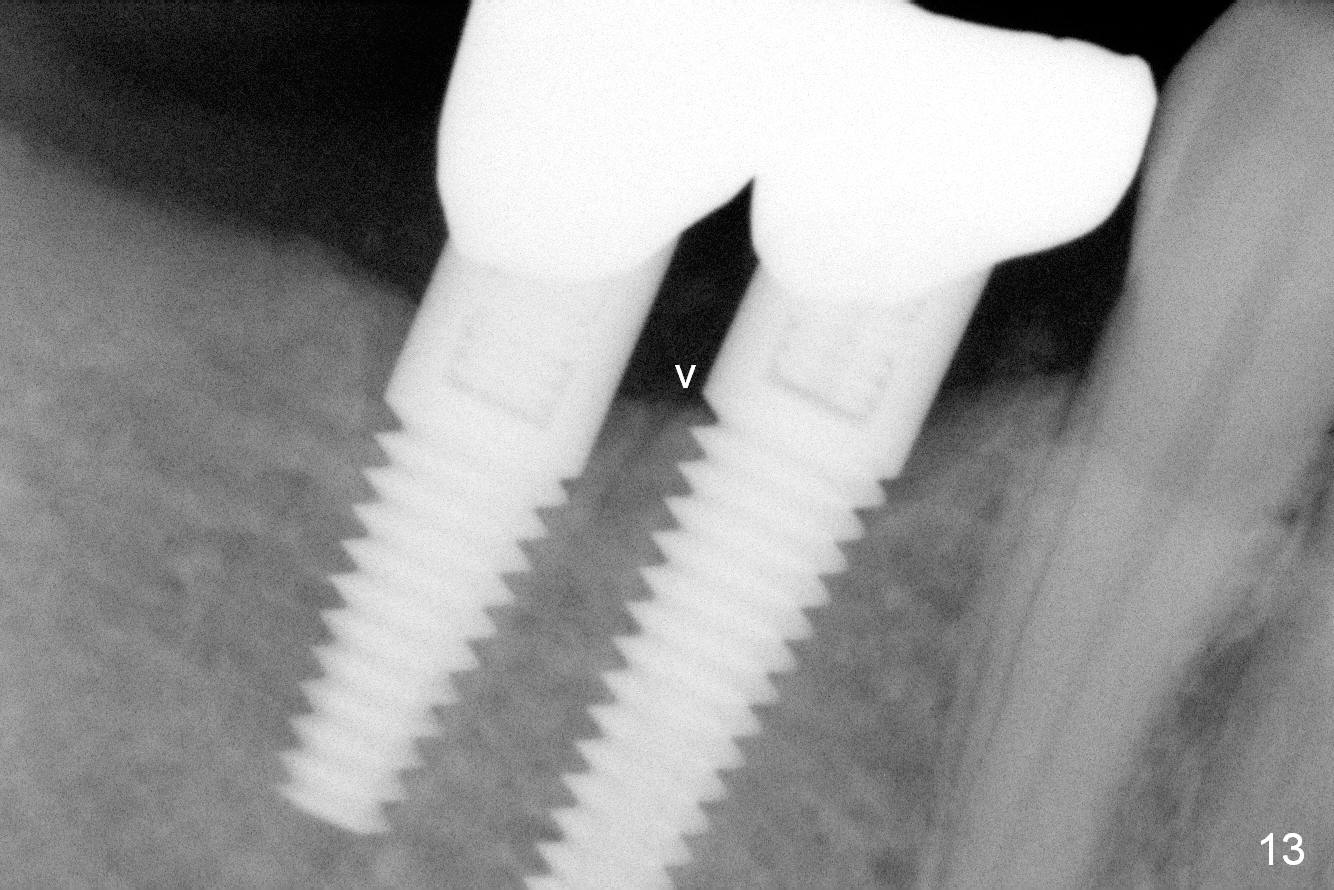
Three months postop, the repositioned implant osteointegrates (Fig.10) and remains lingual in position (Fig.11,12), although there is buccal plate atrophy (Fig.11). Four months post cementation, there is no further bone resorption (Fig.13). Crestal bone loss occurs prior to the 2nd surgery (Fig.4-10). It appears that the adjacent implants should be smaller (4 mm or less).
Return to Lower Premolar Immediate Implant,
Posterior Immediate Provisional, 20,
30
Xin Wei, DDS, PhD, MS 1st edition 11/10/2015, last revision 04/04/2018