
%201%20p.jpg)
.jpg)







|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Two of 2.5 mm 1-Piece Implants M
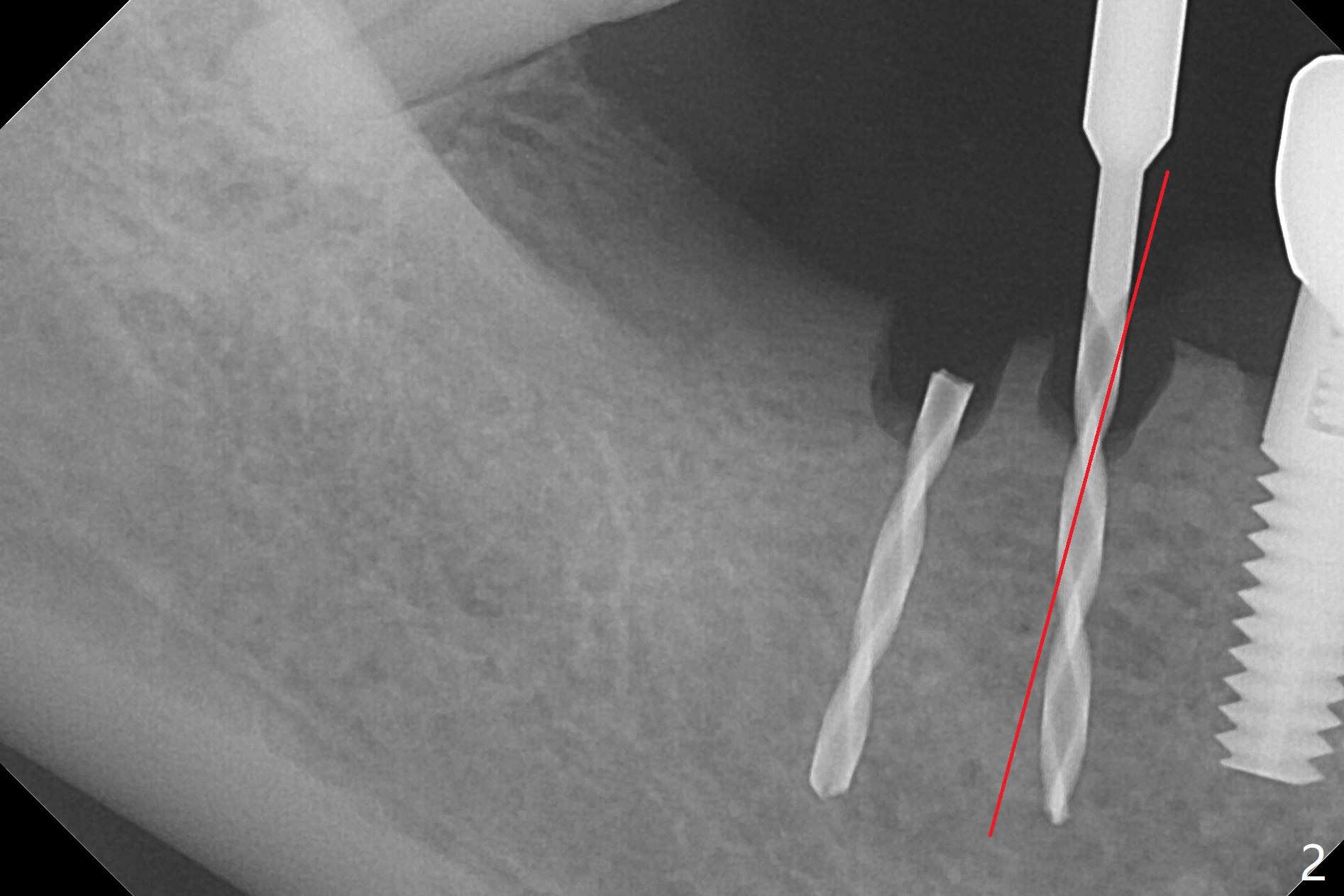
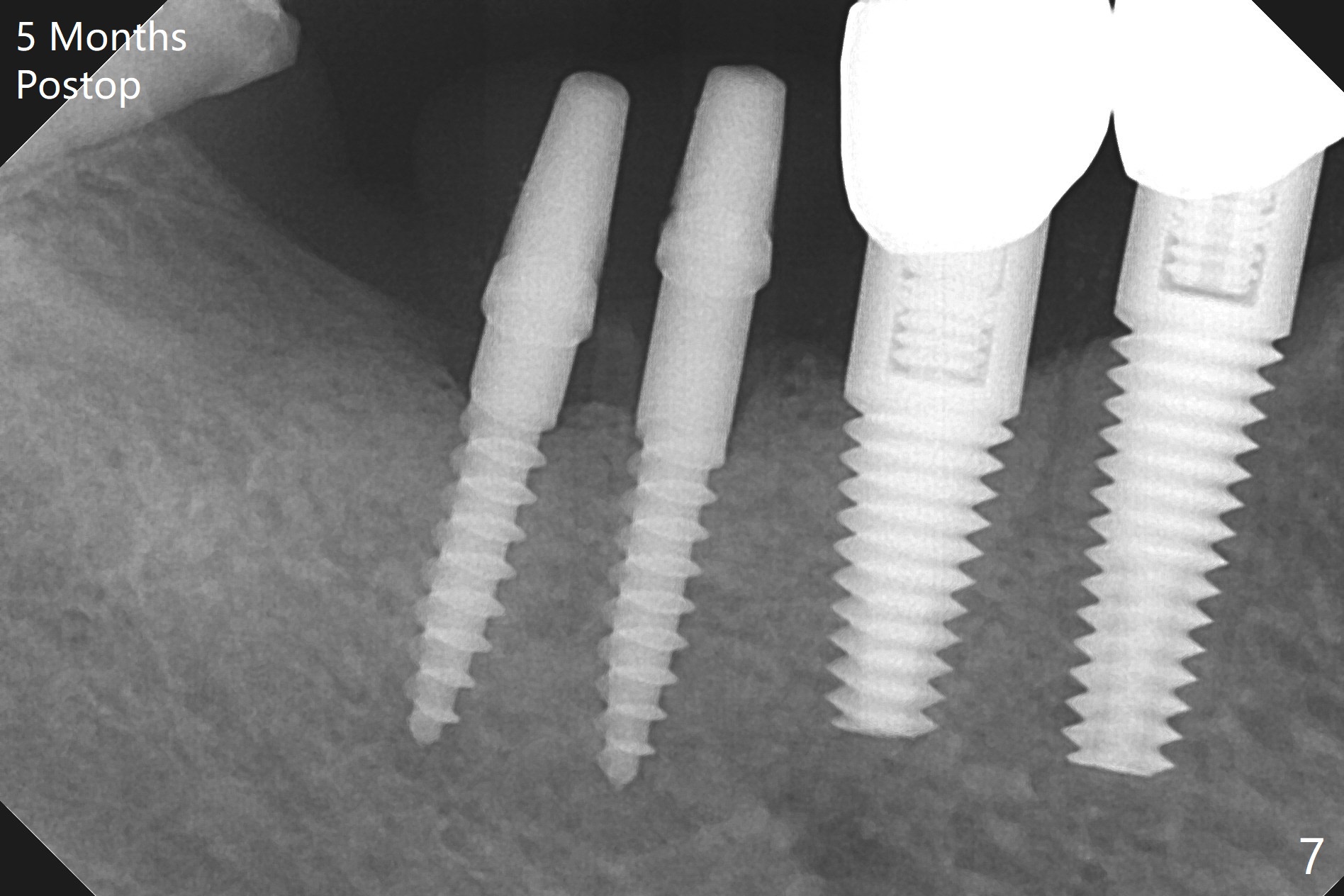
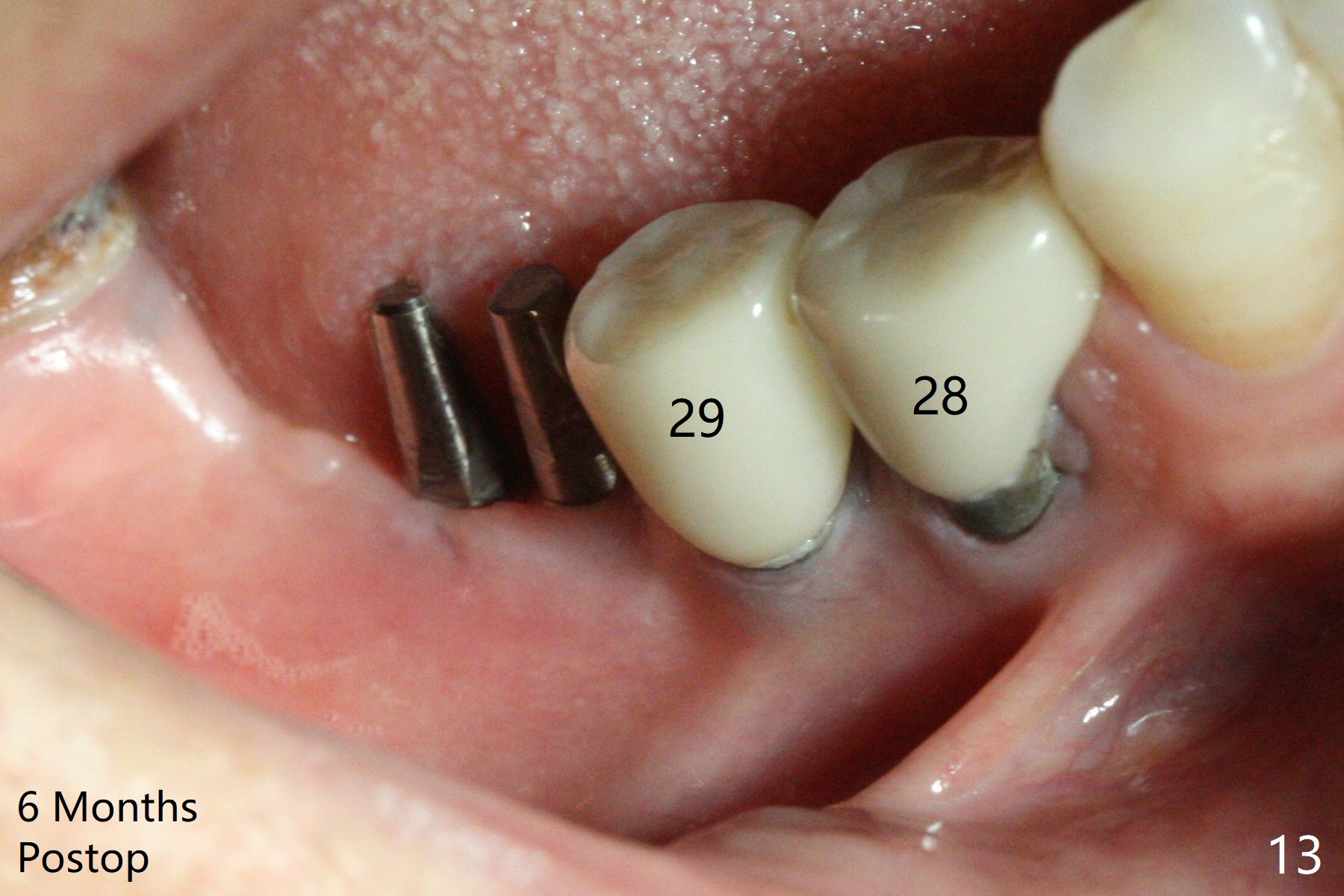
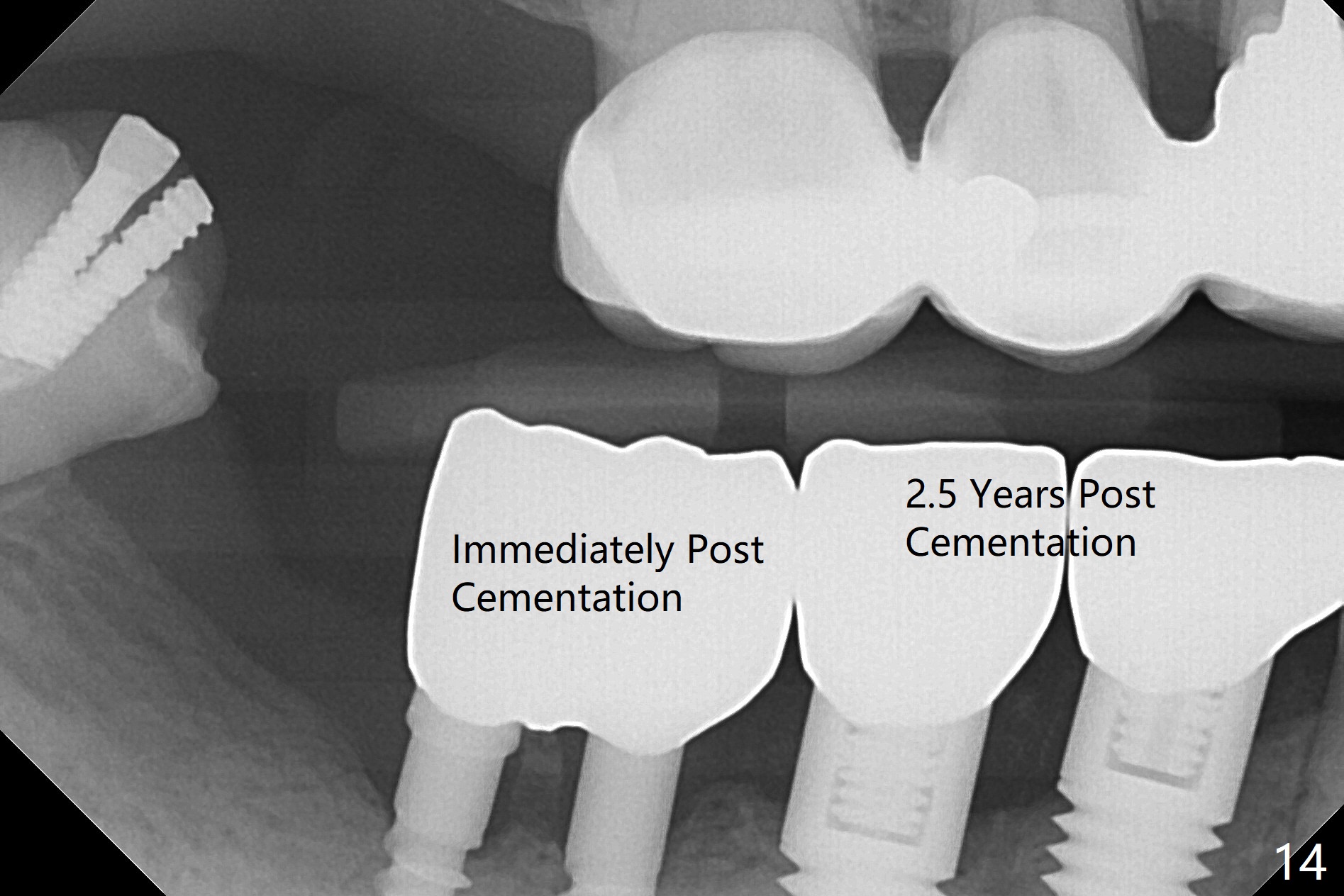
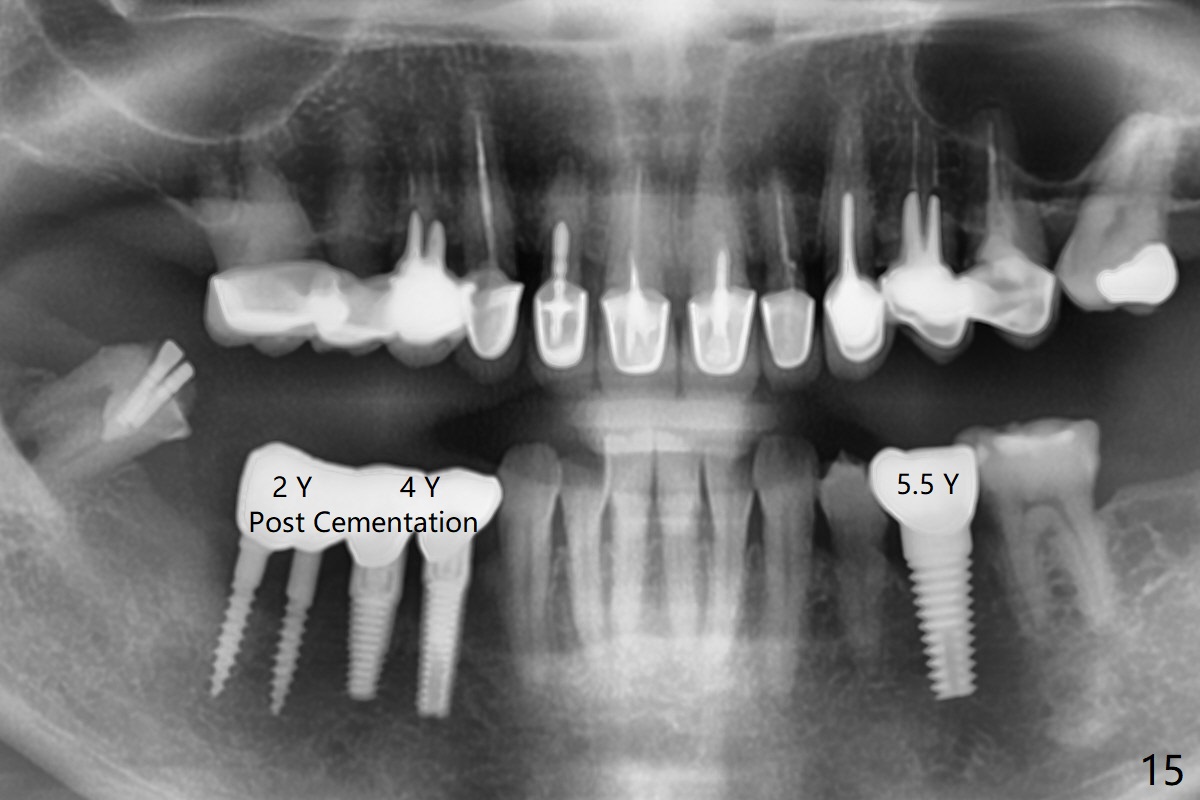
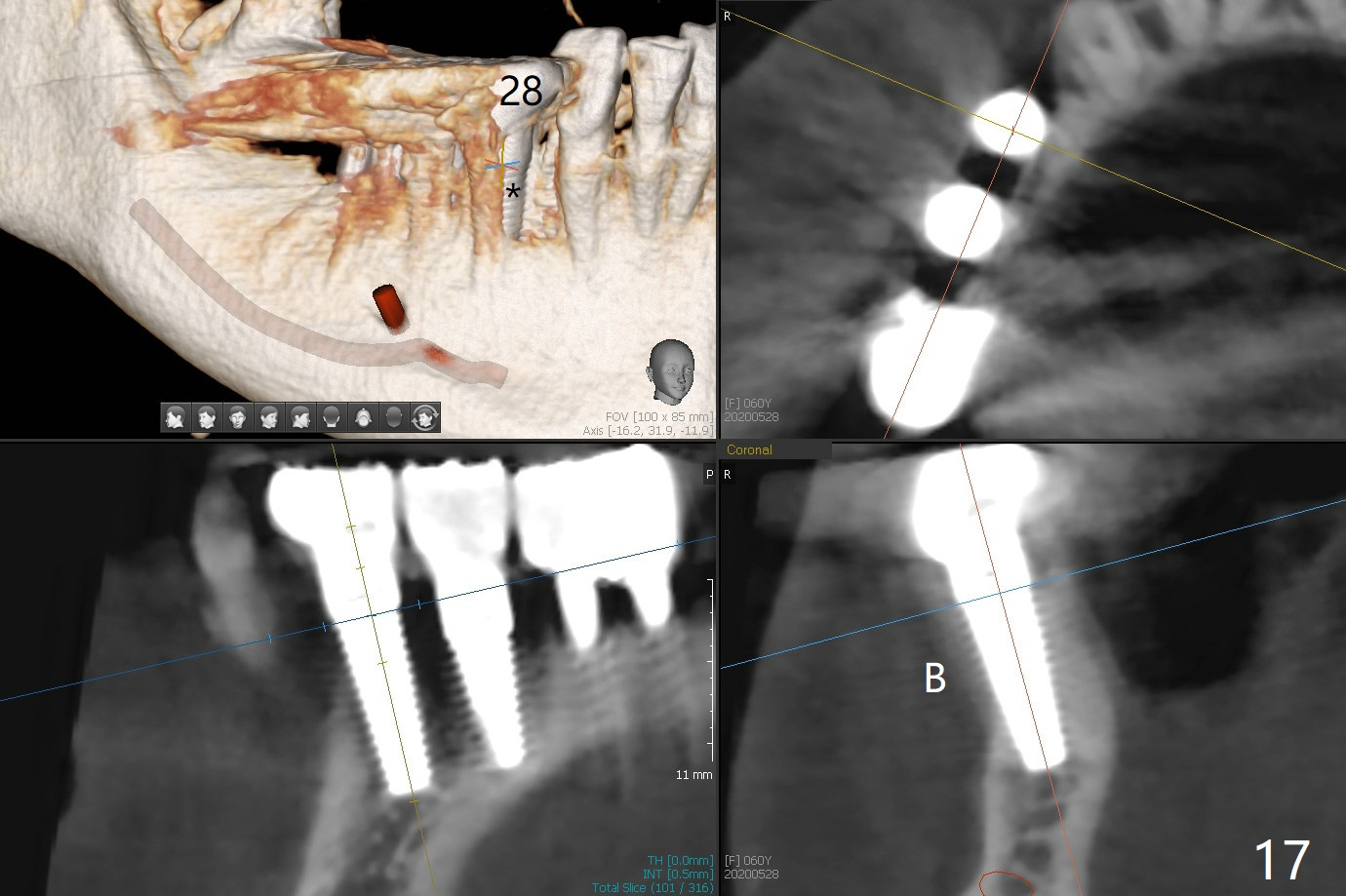
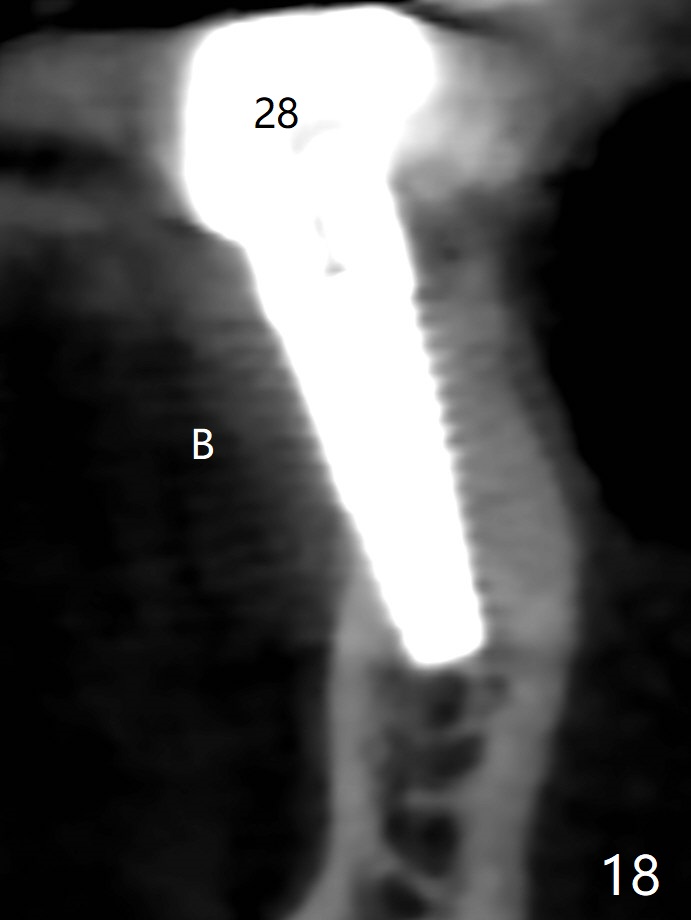
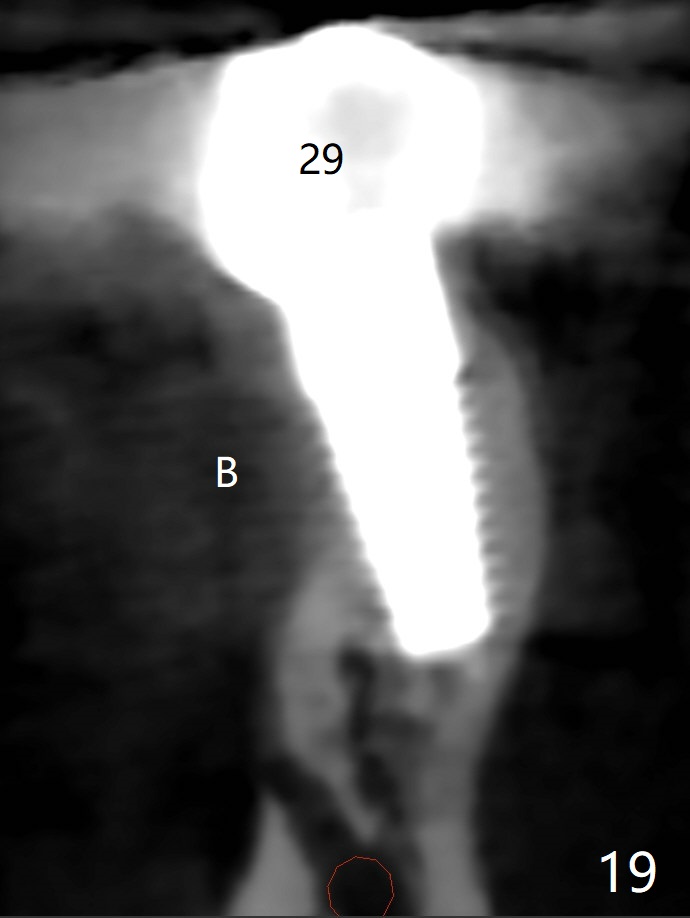
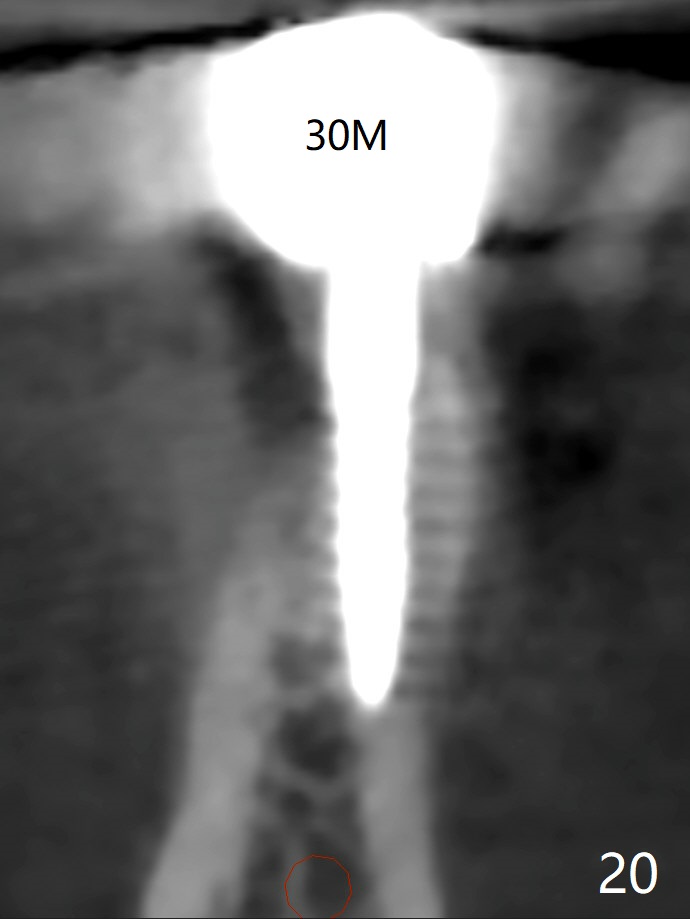
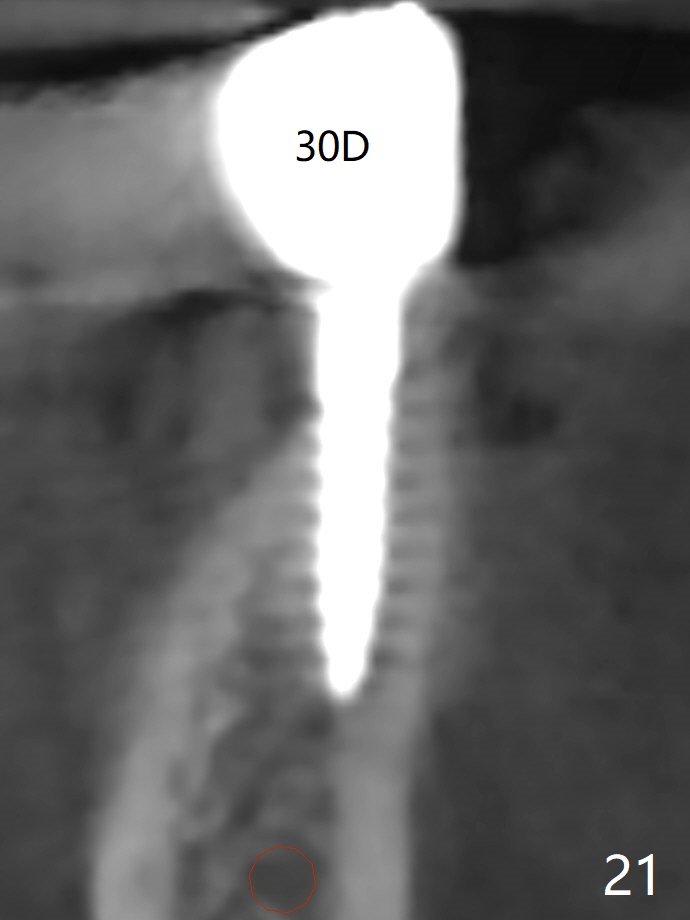
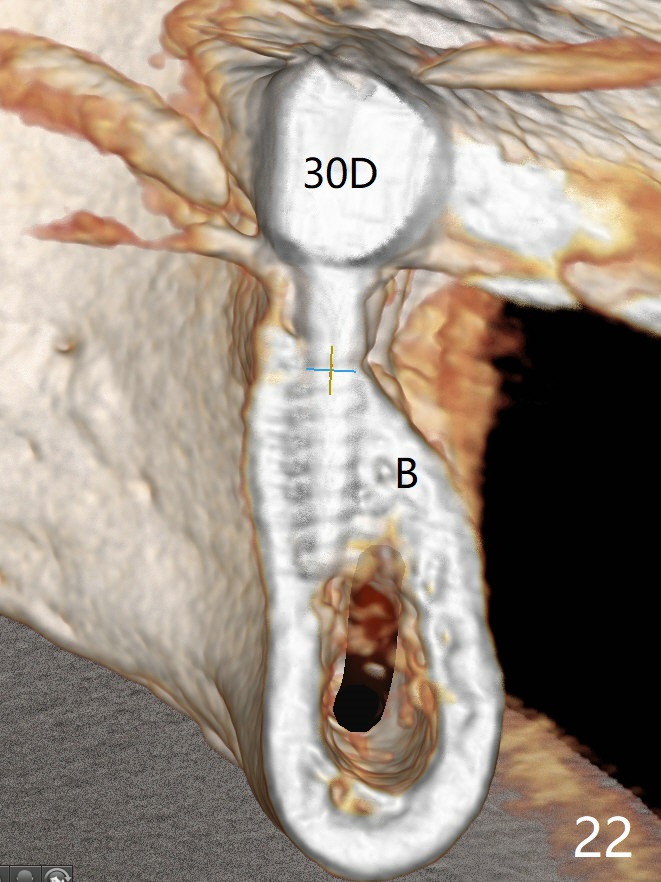
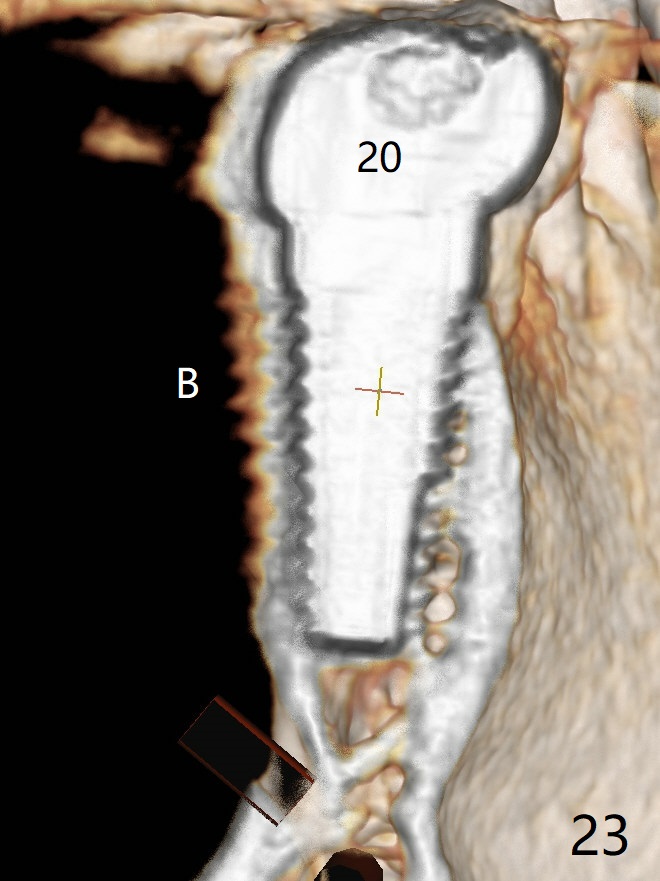
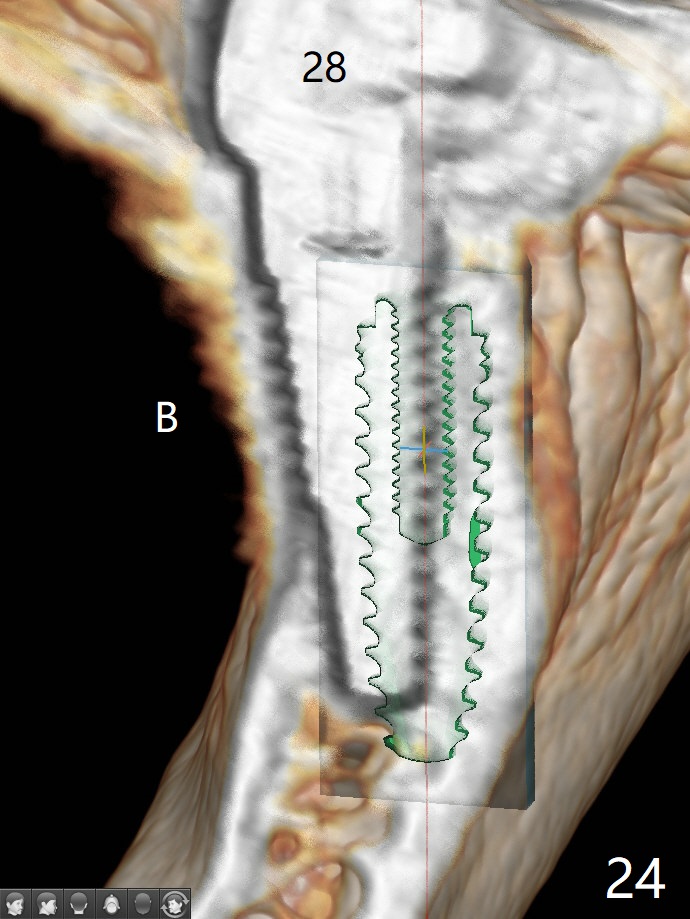
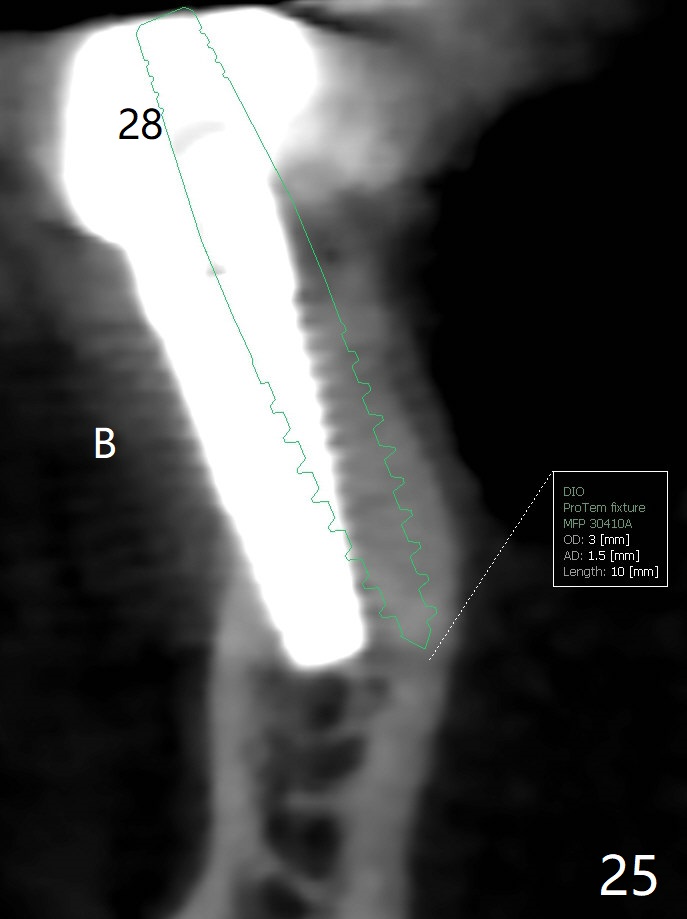
The edentulous ridge at #30 is narrow (Fig.1). After ridge reduction, osteotomy is initiated with 1.2 mm drill for 10 mm; the mesial osteotomy is to be changed (Fig.2 red line). Using a 1.2 mm drill placed in the distal osteotomy (Fig.3 D), the mesial osteotomy changes in trajectory with subsequent placement of a 2.5x10(4) mm 1-piece implant. Since the mesial implant is high in occlusion, the cuff of the distal implant is changed to be 2 mm (Fig.4 (shorter black line)). Panoramic X-ray is taken to show no violation of the Inferior Alveolar Canal (Fig.5 red dashed line). These two 1-piece implants are slightly lingually placed (Fig.6). The crestal bone around the implants resorbs without thread exposure 5 months postop (Fig.7). Impression is taken for a splinted crown (Fig.8-12). There is no metal show around the 2.5 mm 1-piece implants 6 months postop (advantage) vs. that at #28 and 29 (Fig.13). Bitewing is taken post cementation to determine whether residual cement is present (Fig.14). There is periodic swelling and pain in the lower right quadrant 2 years post cementation (Fig.15). In fact periimplantitis appears to have developed at #28 (Fig.16) with loss of the buccal bone (Fig.17,18). The buccal bone loss is less at #29 (Fig.19) and #20 (Fig.23) and no at #30 mesial and distal implants (Fig.20,21). A much smaller implant will be placed lingually at #28 immediate (Fig.24,25).
Return to
Lower
Molar Immediate Implant,
IBS,
20,
28/29
No
Caries
6
即种全程
Xin Wei, DDS, PhD, MS 1st edition 10/05/2017, last revision 07/02/2021