
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
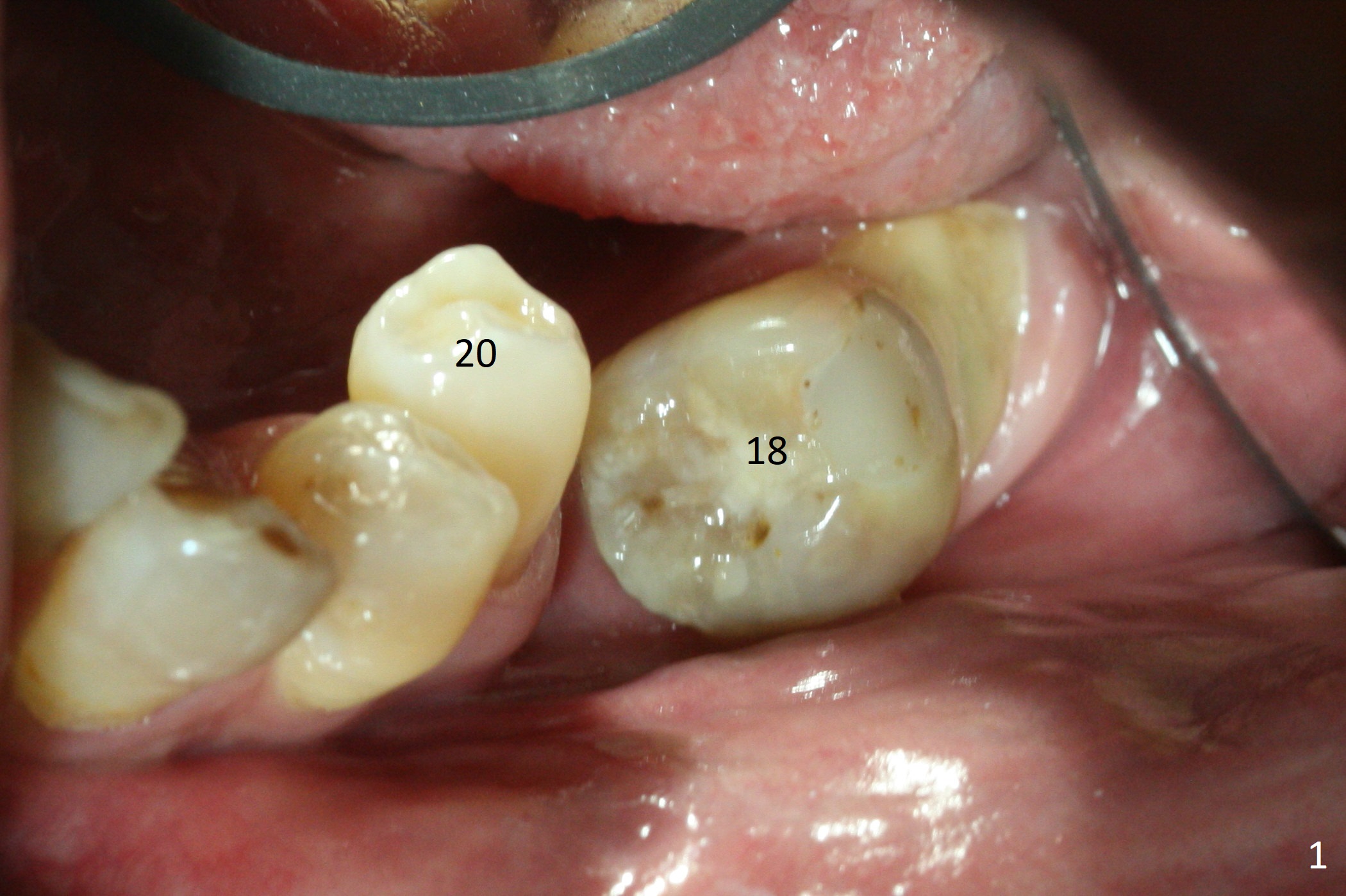
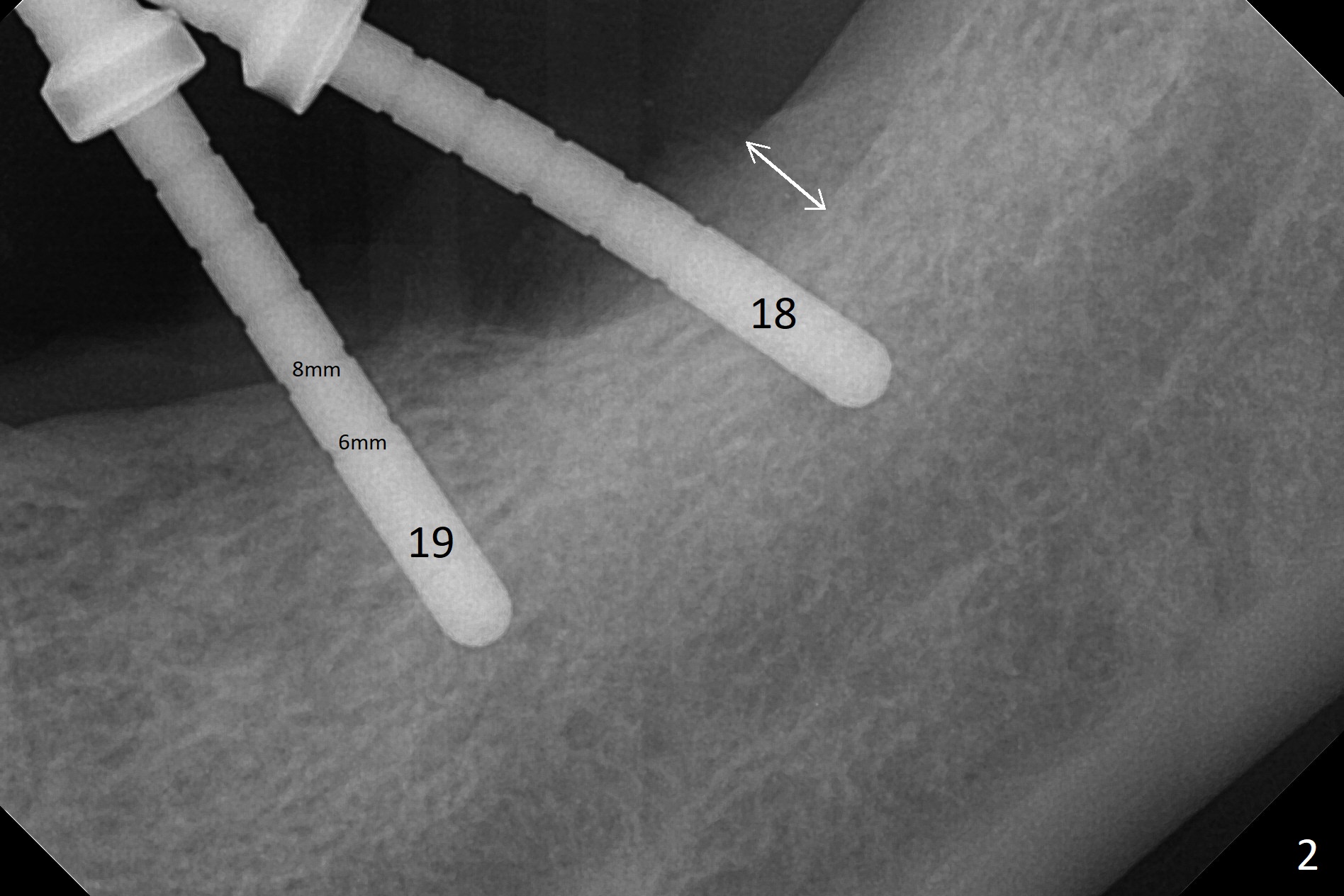
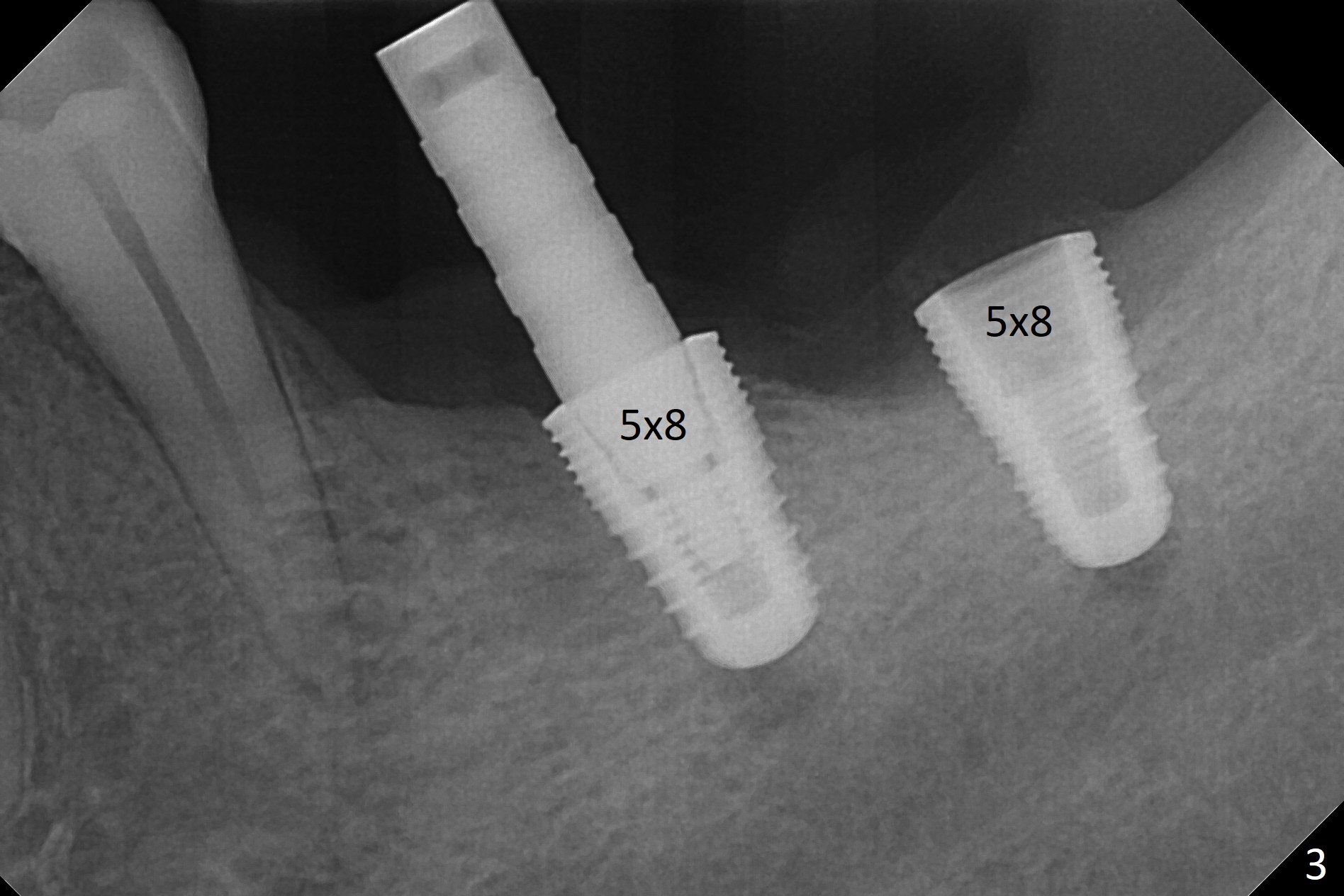
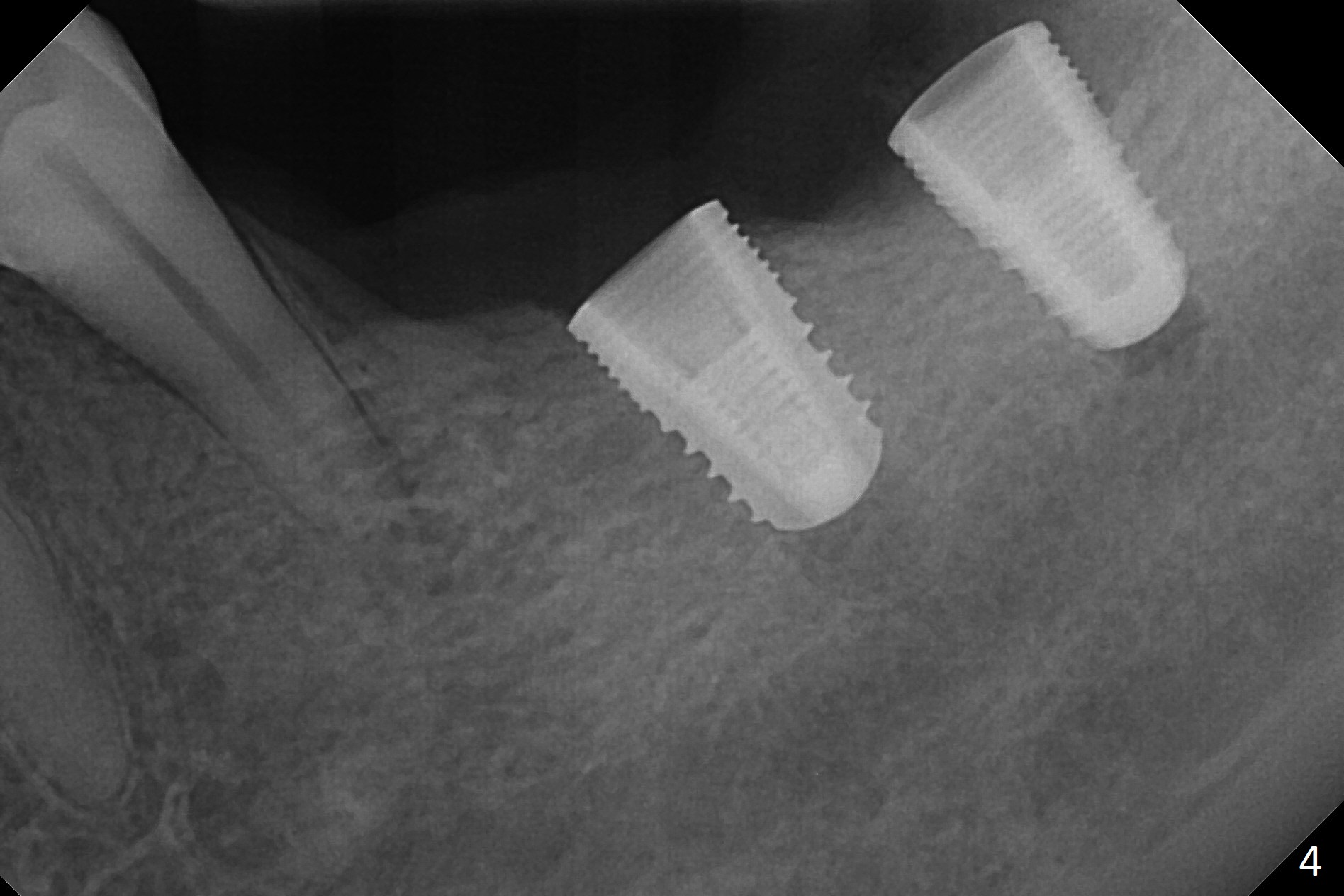
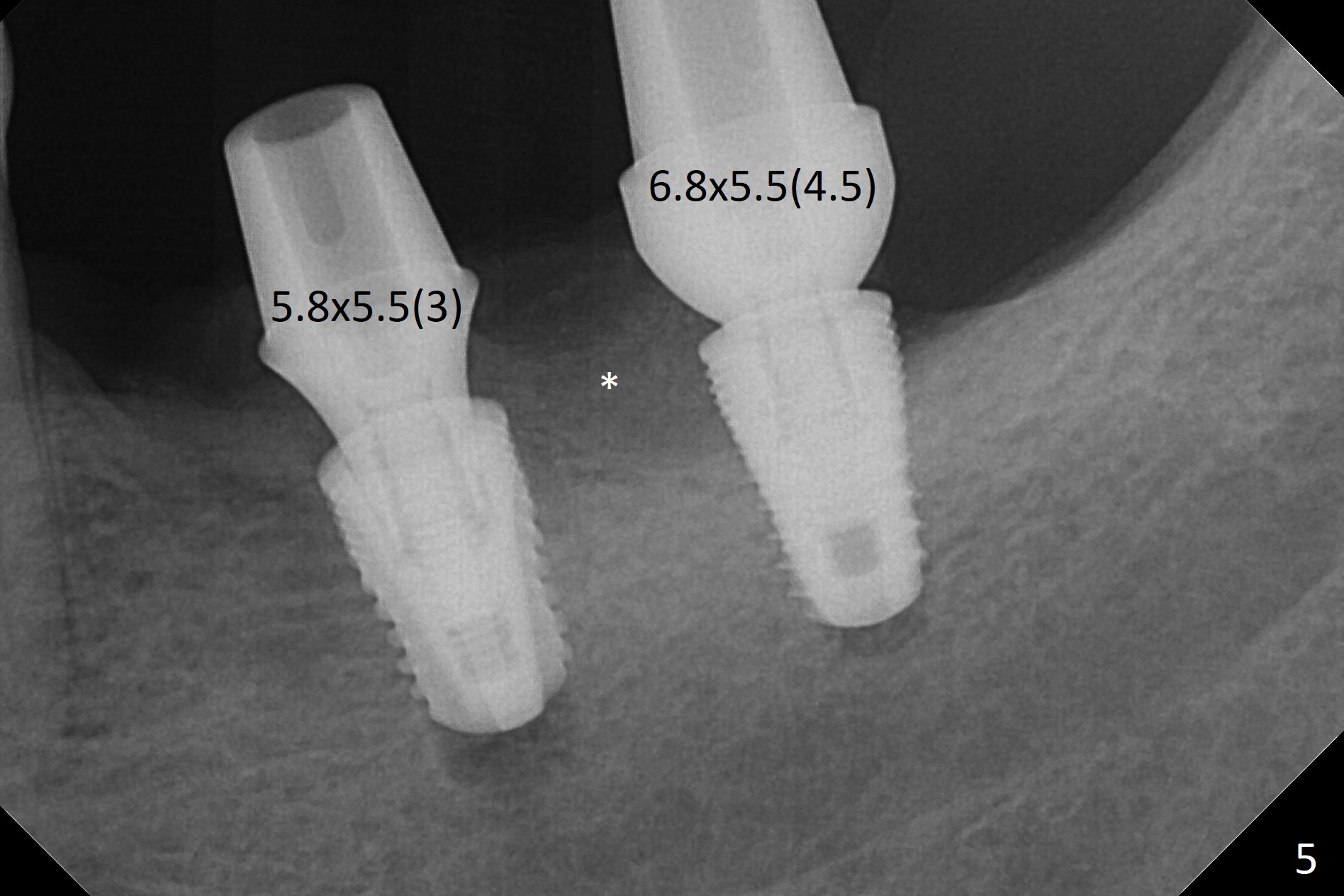
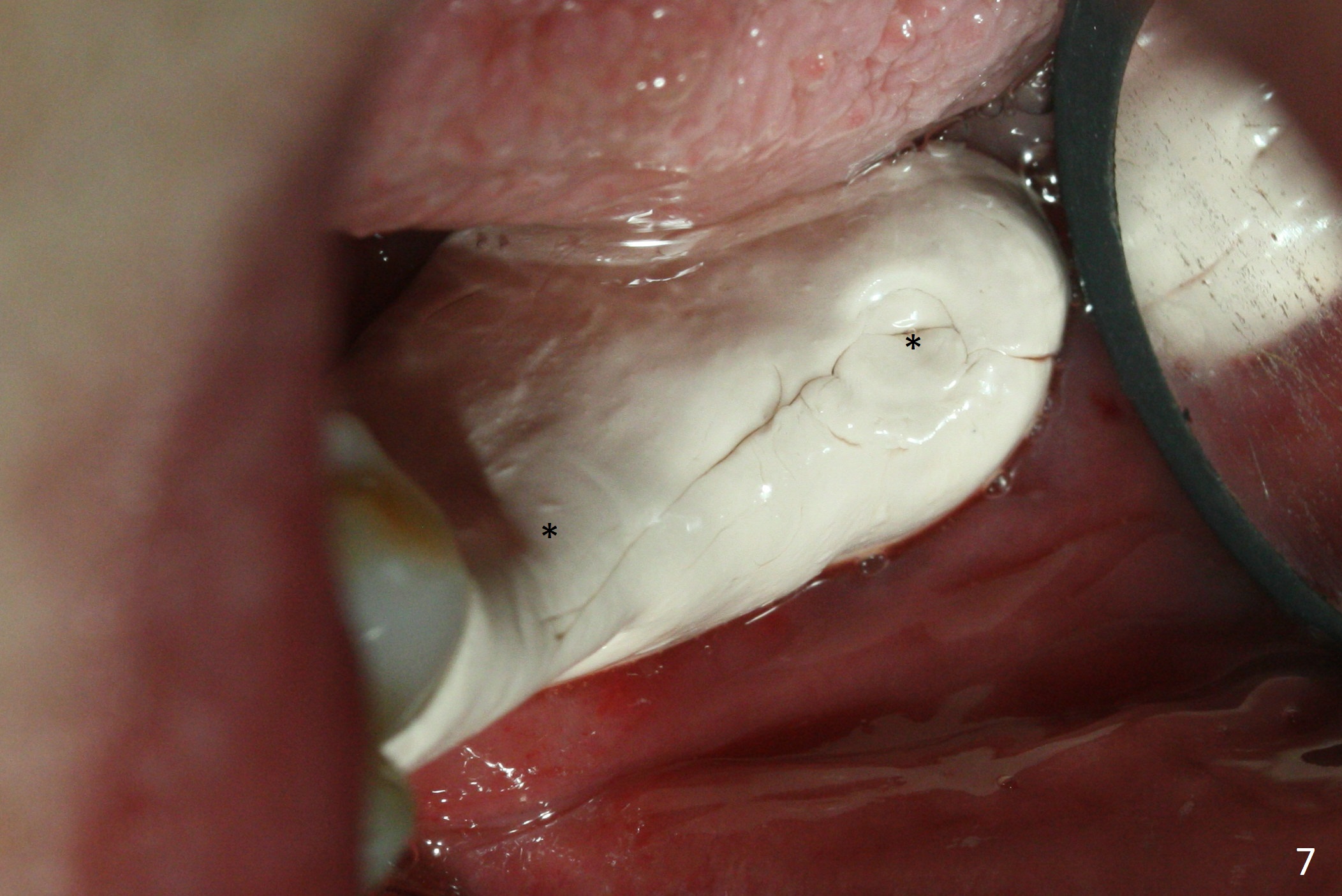
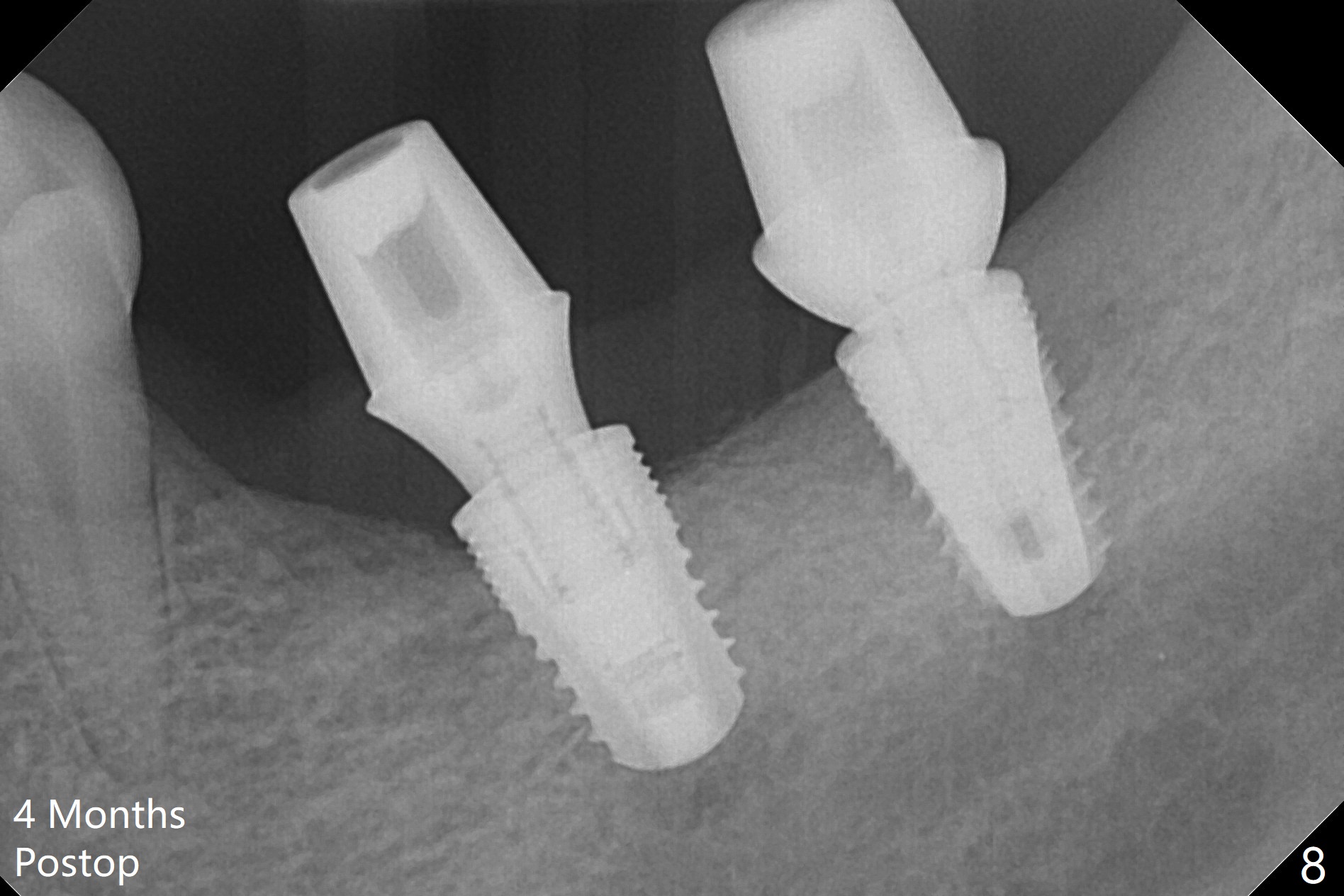
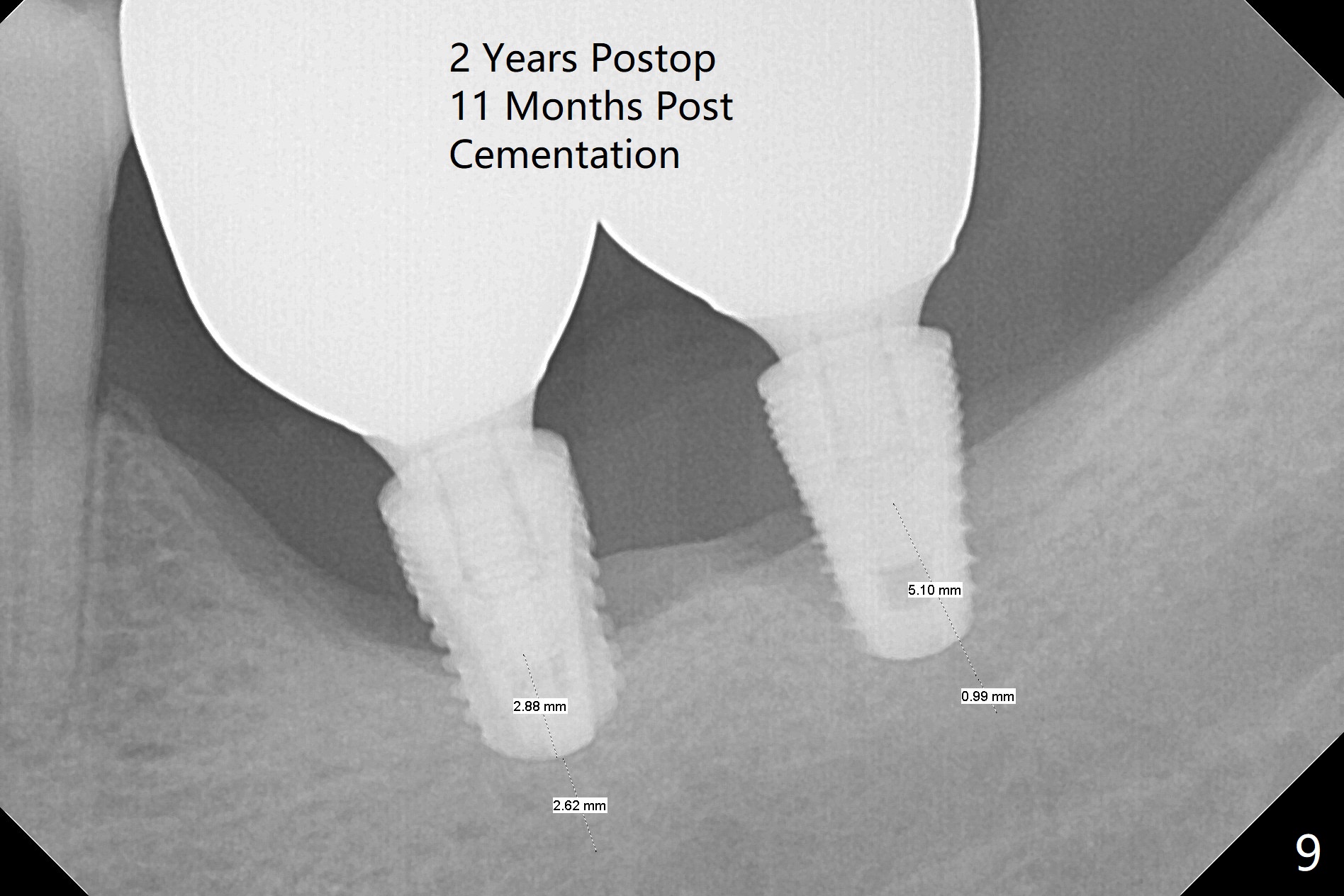
Buccolingual Plate Discrepancy
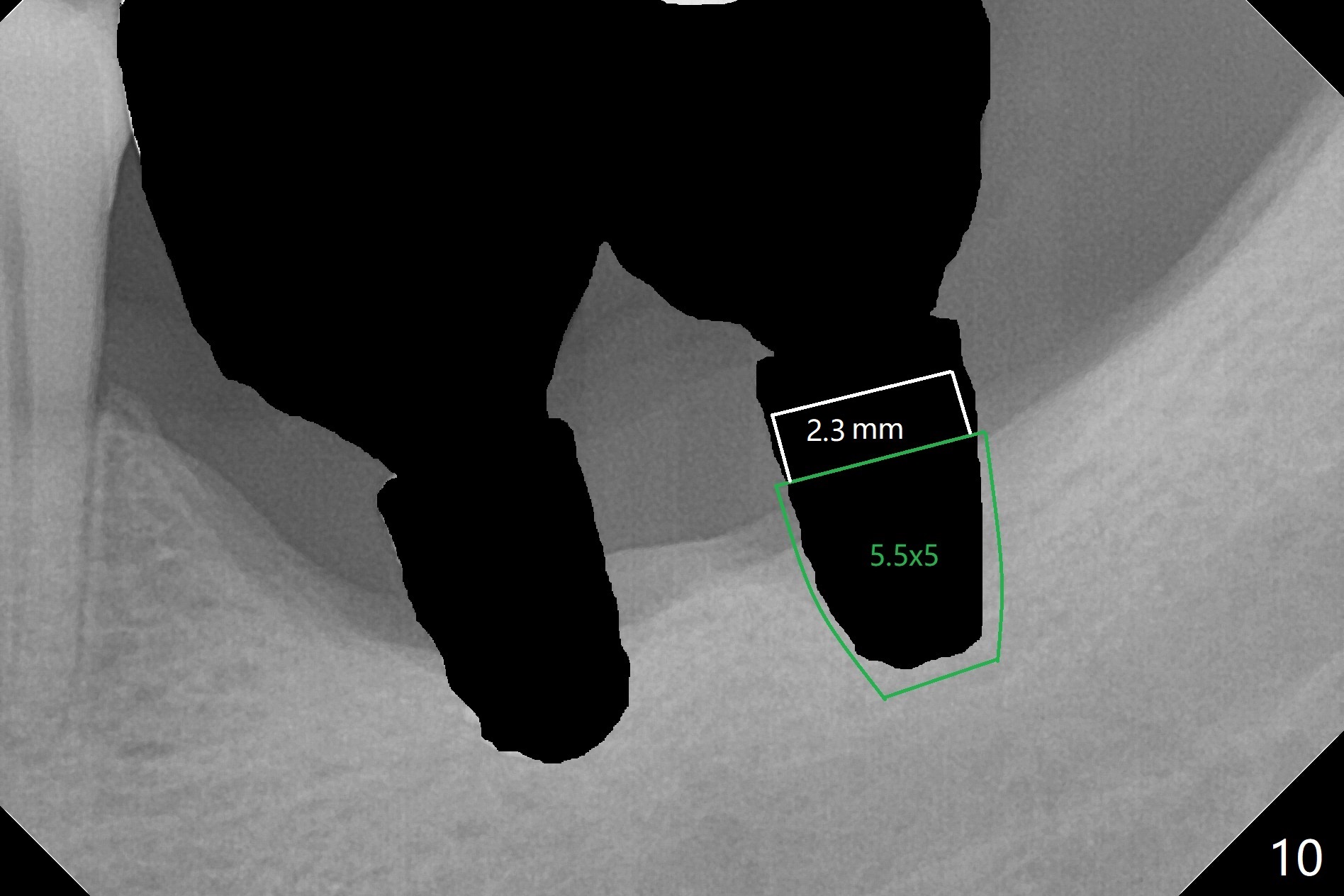
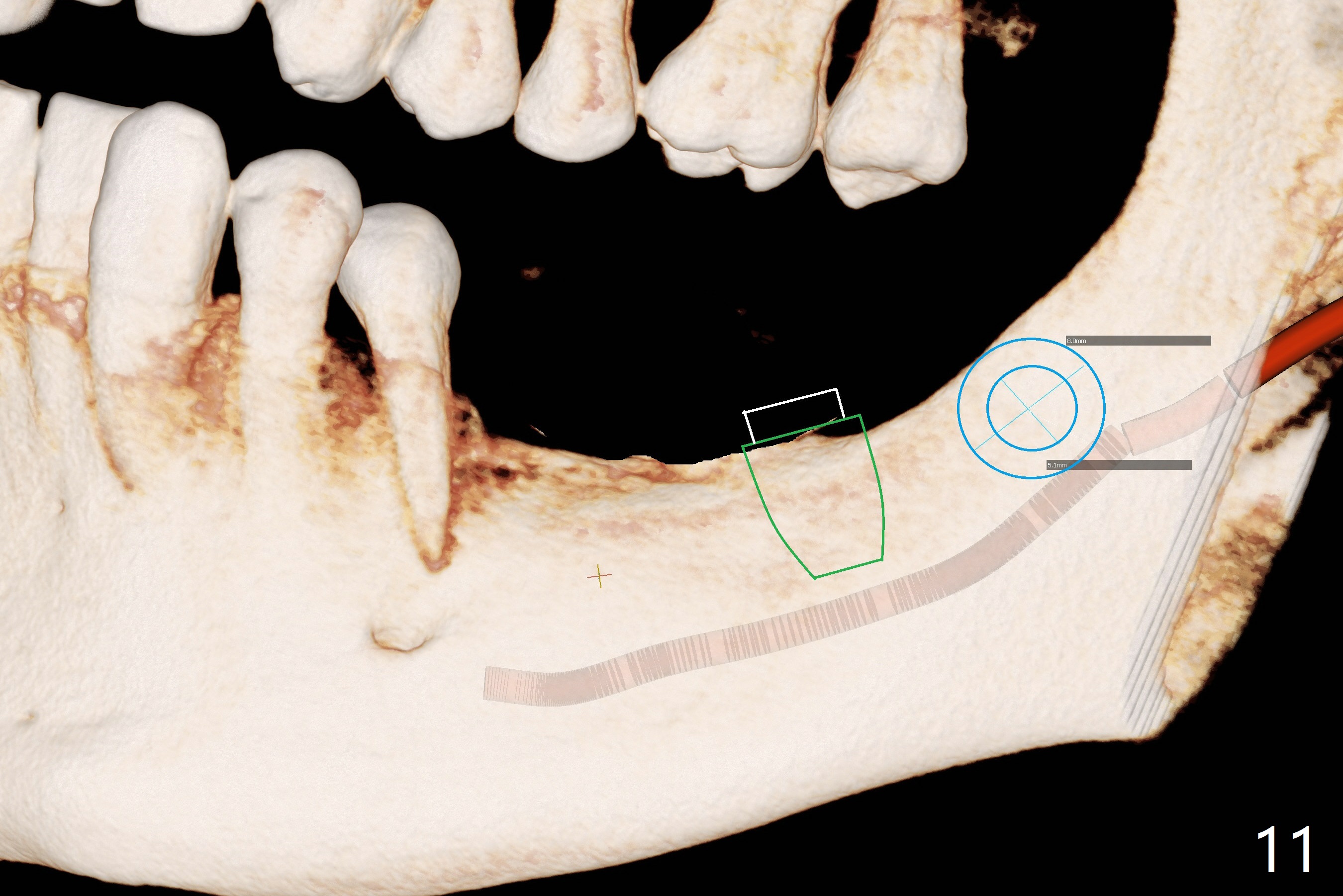
Preop photo shows severe mesial tilt of the tooth #18 (Fig.1). After extraction, the osteotomy is established in the apical end of the socket, where the buccolingual width is limited. It appears that an extra wide implant (5.9 mm) may perforate one of buccolingual plates. On the other hand, the buccal plate (Fig.2 double arrows) is intact and approximately 2 mm tall, whereas the lingual one is thin and lower. Initial osteotomy confirms that bone heights at #18 and 19 are 6 and 8 mm, respectively. Counting 2 mm of the buccal plate and bone graft lingually, a 8 mm long implant may be a practical option at the site of #18. After initial placement of two of 5x8 mm SM implants (Fig.3), the depth of the implant at #19 is adjusted twice (Fig.4,5). With placement of autogenous and allograft (Vanilla, Fig.5 *)) and abutments, a piece of cotton pellet is placed in each abutment well (access, Fig.6 *). Periodontal dressing is applied to the abutment wells for additional retention (Fig.7 *). Due to local poor oral hygiene, splinted provisional is fabricated 4 months postop (Fig.8) in preparation for limited orthodontic uprighting the tooth #20. The patient has pain with mastication at #18 eleven months post cementation (Fig.9). It appears that both of the implants should be removed with immediate replacement and bone graft. Prepare 4 PRF and sticky bone. The new implant will be 5.0 or 5.5x5 mm (Fig.10 green) with 2.3 mm platform (white). A block graft will be harvested from the ipsilateral ramus using 9/8 and 6/5 mm trephine burs for 2-3 mm in depth (Fig.11 blue). The ring graft will be seated around the platform over the implant (Fig.12).
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS,
#3,4
Trajectory II
Xin Wei, DDS, PhD, MS 1st edition 11/02/2017, last revision 04/21/2020