


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Implant in 3rd Molar?
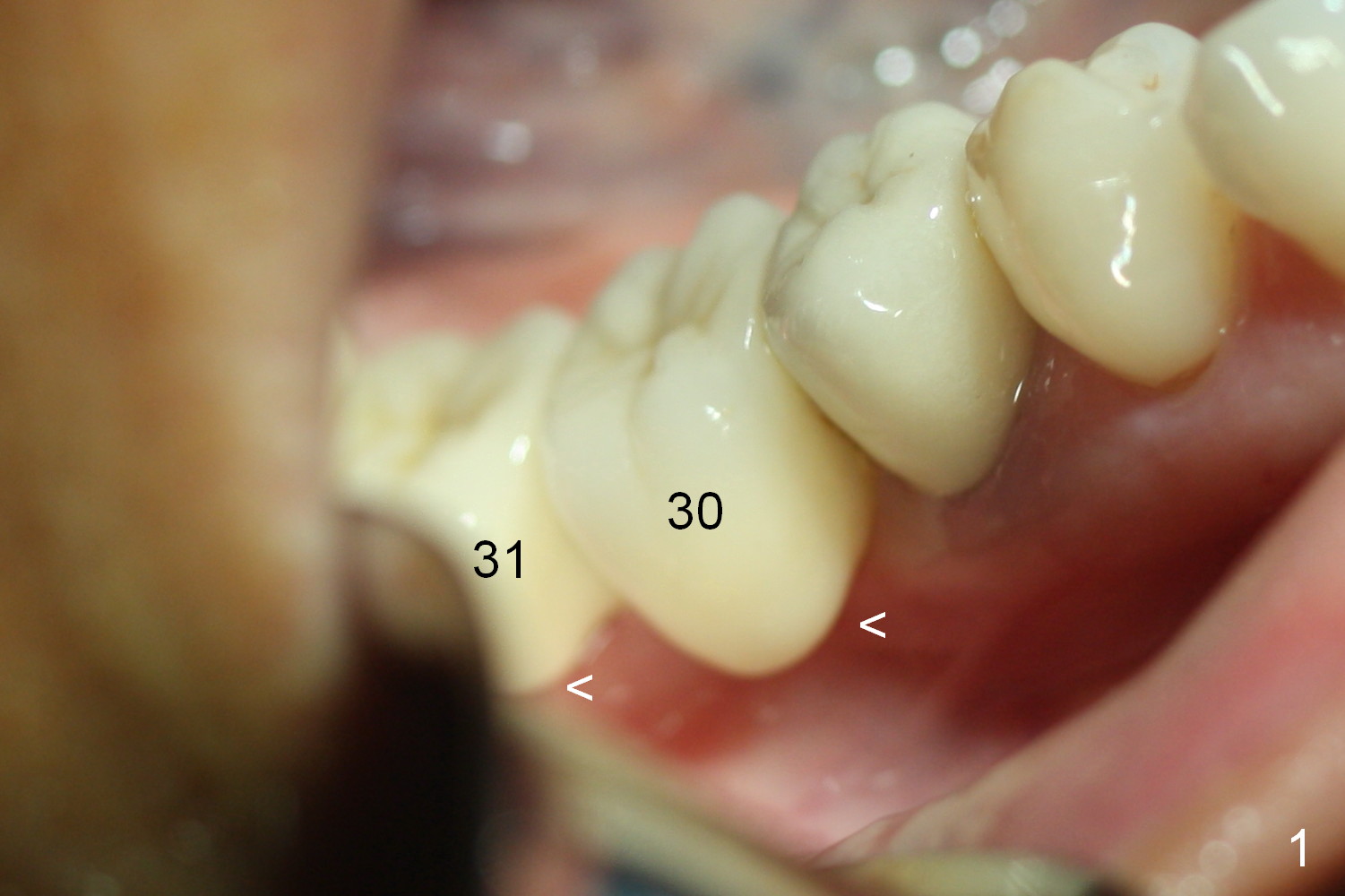
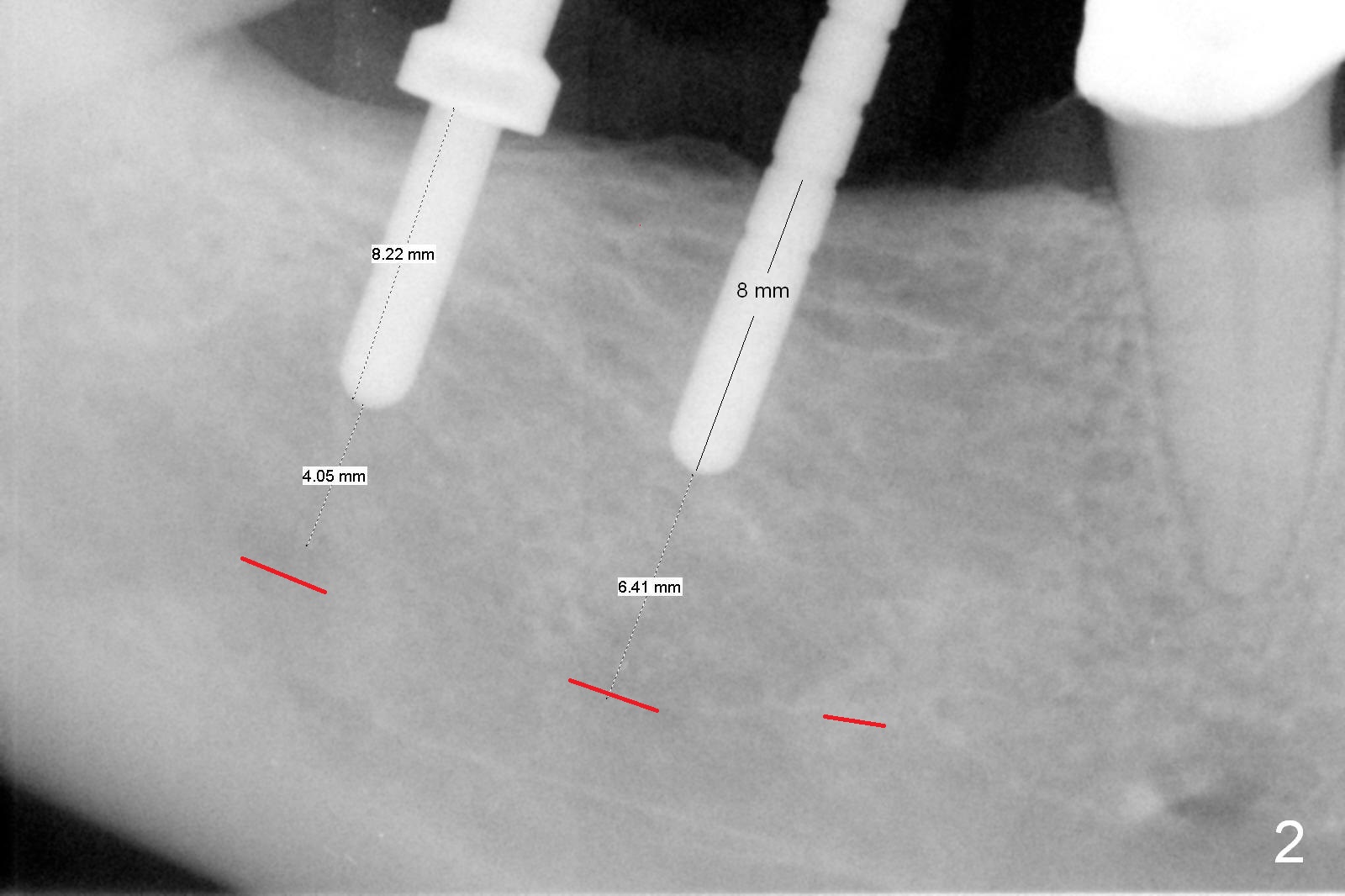
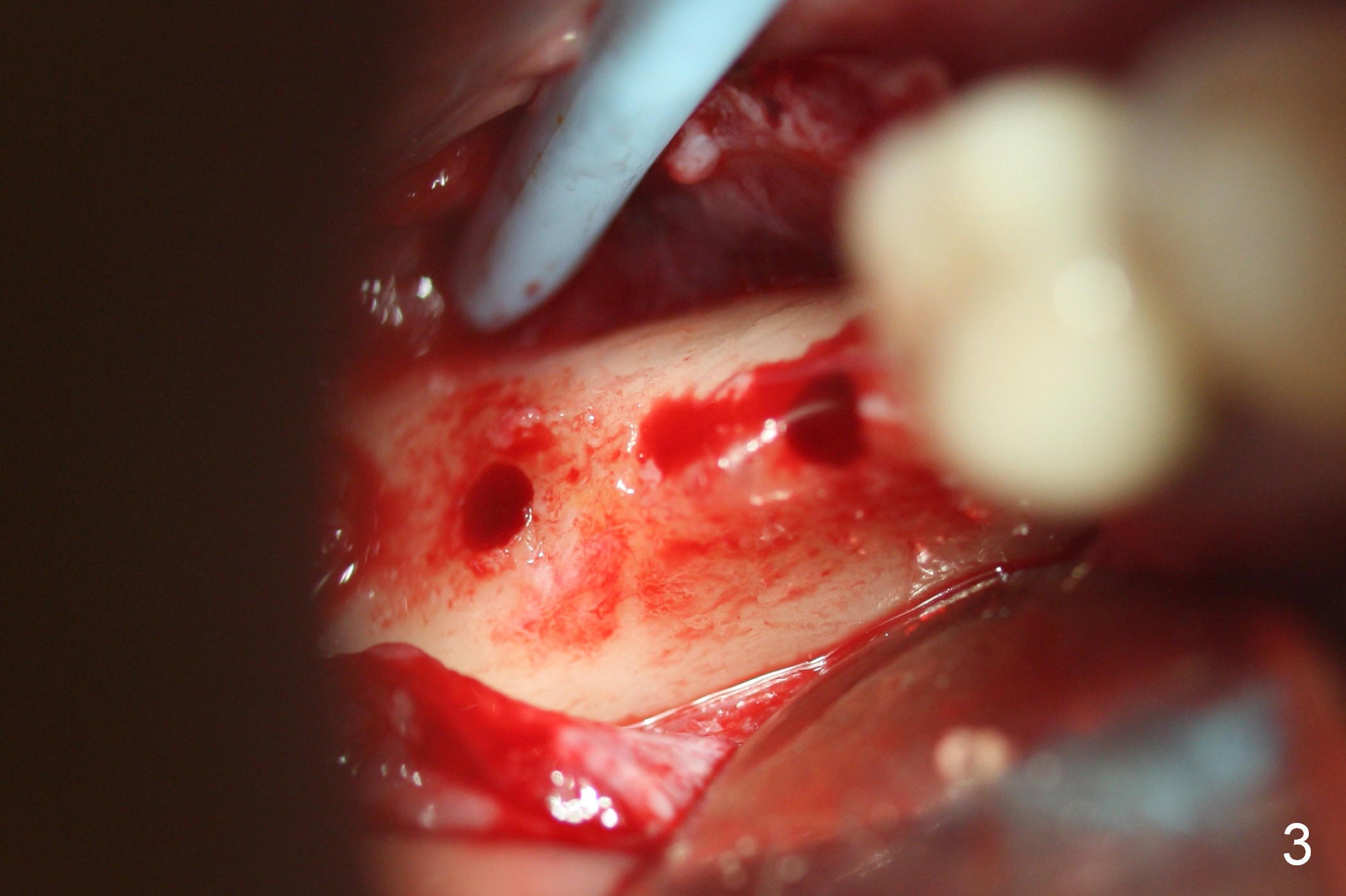
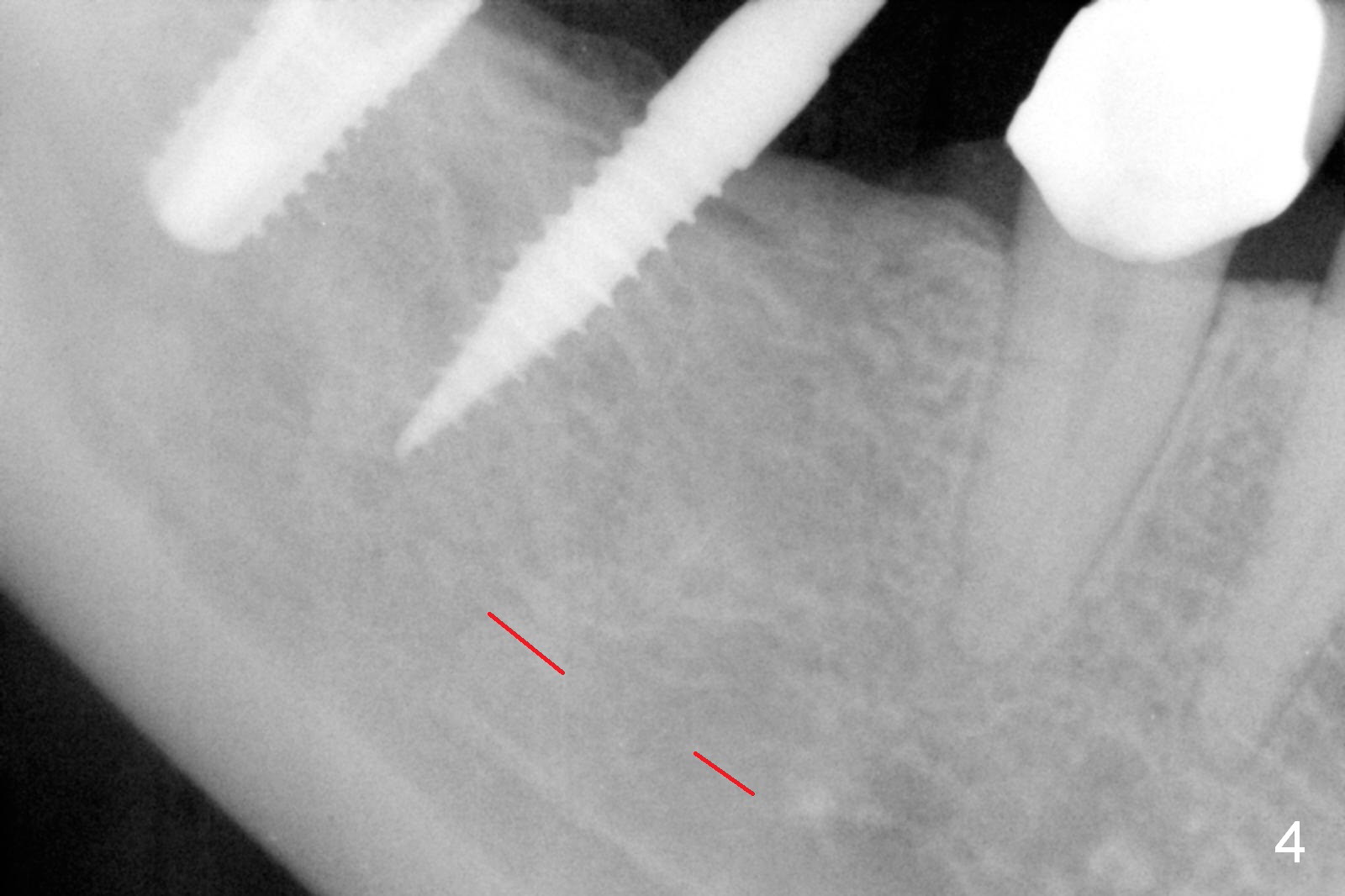
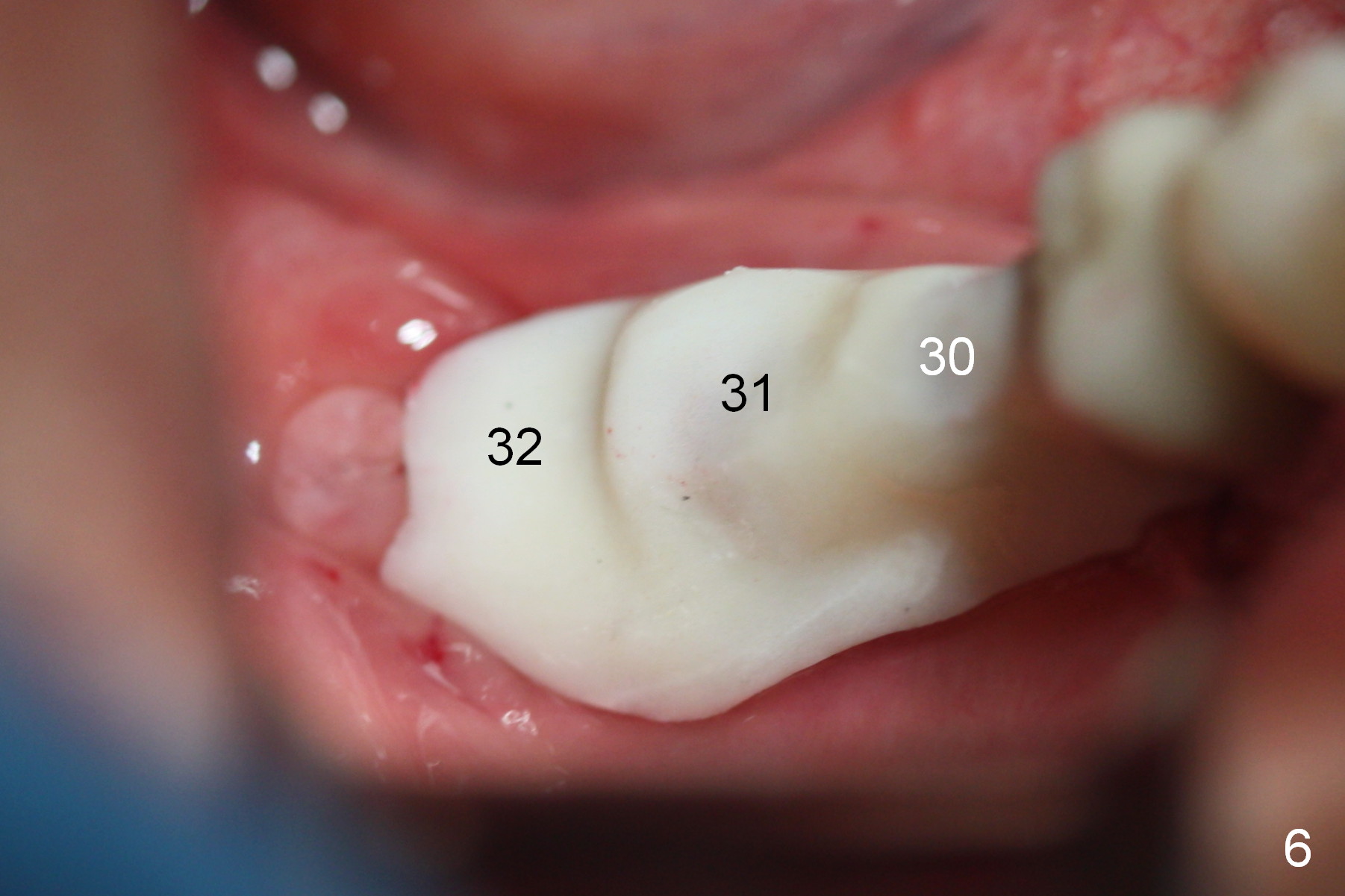
A preop photo shows different shape of pontics at #30 and 31 (Fig.1 <), suggesting different width of the edentulous ridge. Two of 8 mm parallel pins are inserted for position and trajectory (Fig.2 (red dashed line: the superior border of the Inferior Alveolar Canal). When they are removed from the osteotomy sites, the narrow ridge at #30 is shown (Fig.3). A 3x12 mm 1-piece implant is placed at #30, while a 4.5x10 mm 2-piece one at #31 (Fig.4,5). It appears that it is necessary to place an implant at #32, since the tooth #1 is present (Fig.5). The suggestion is rejected by the patient due to finance. After extraction of the tooth #32 and insertion of collagen plug, an immediate splinted provisional is fabricated to cover the #32 socket as well (Fig.6). The provisional is modified (to remove the portion that covers #32 socket) 3-4 weeks postop.
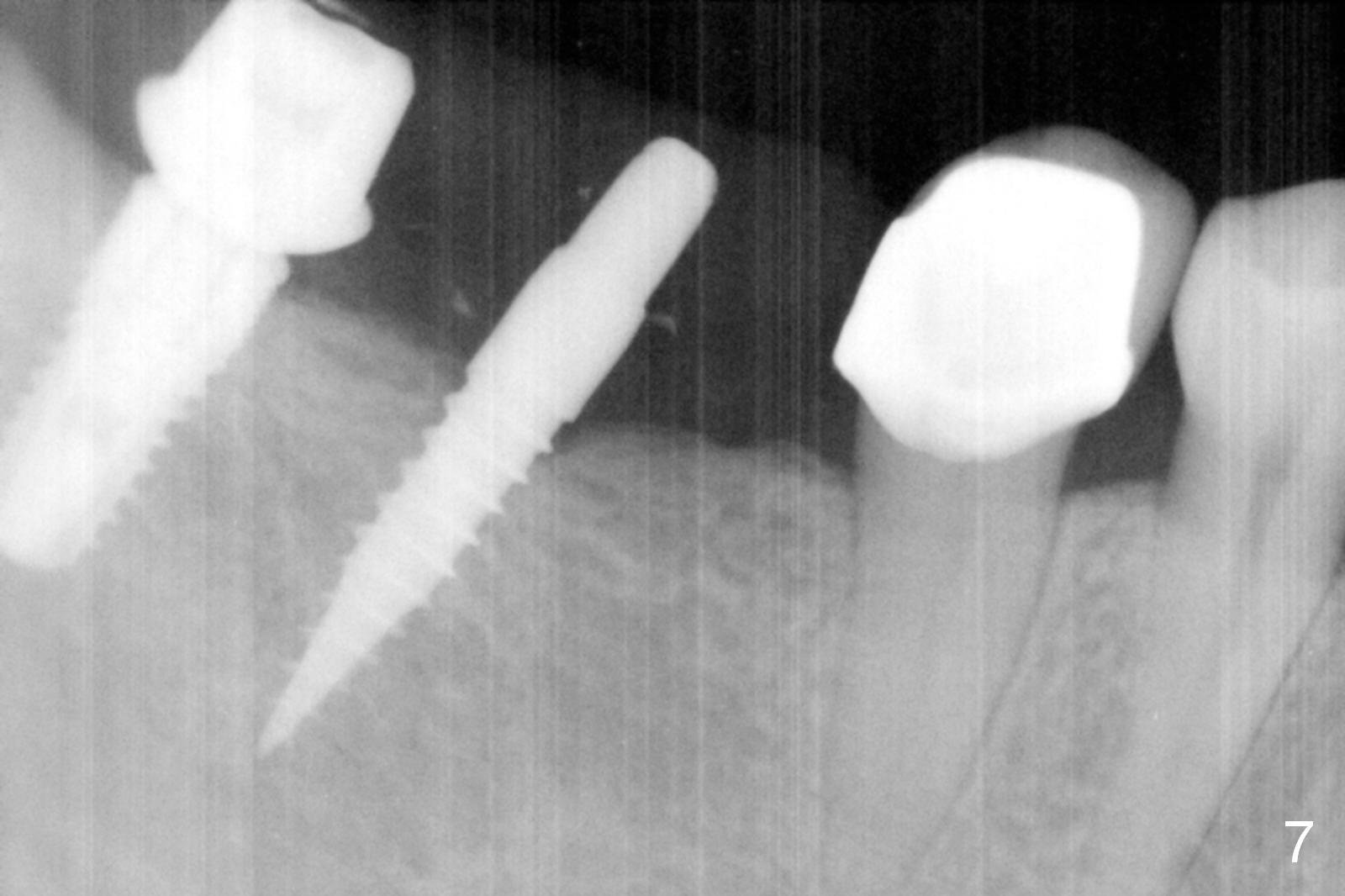
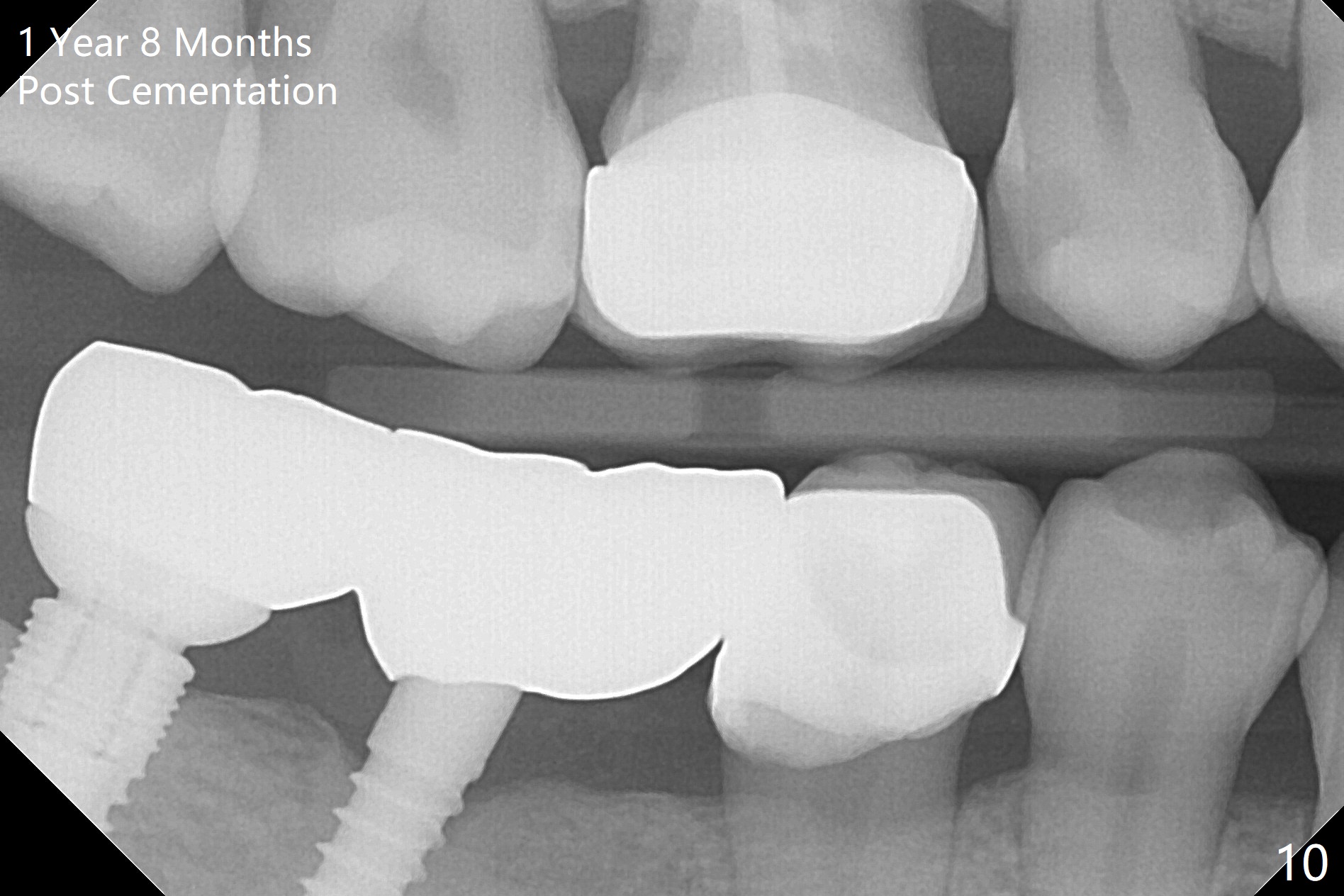
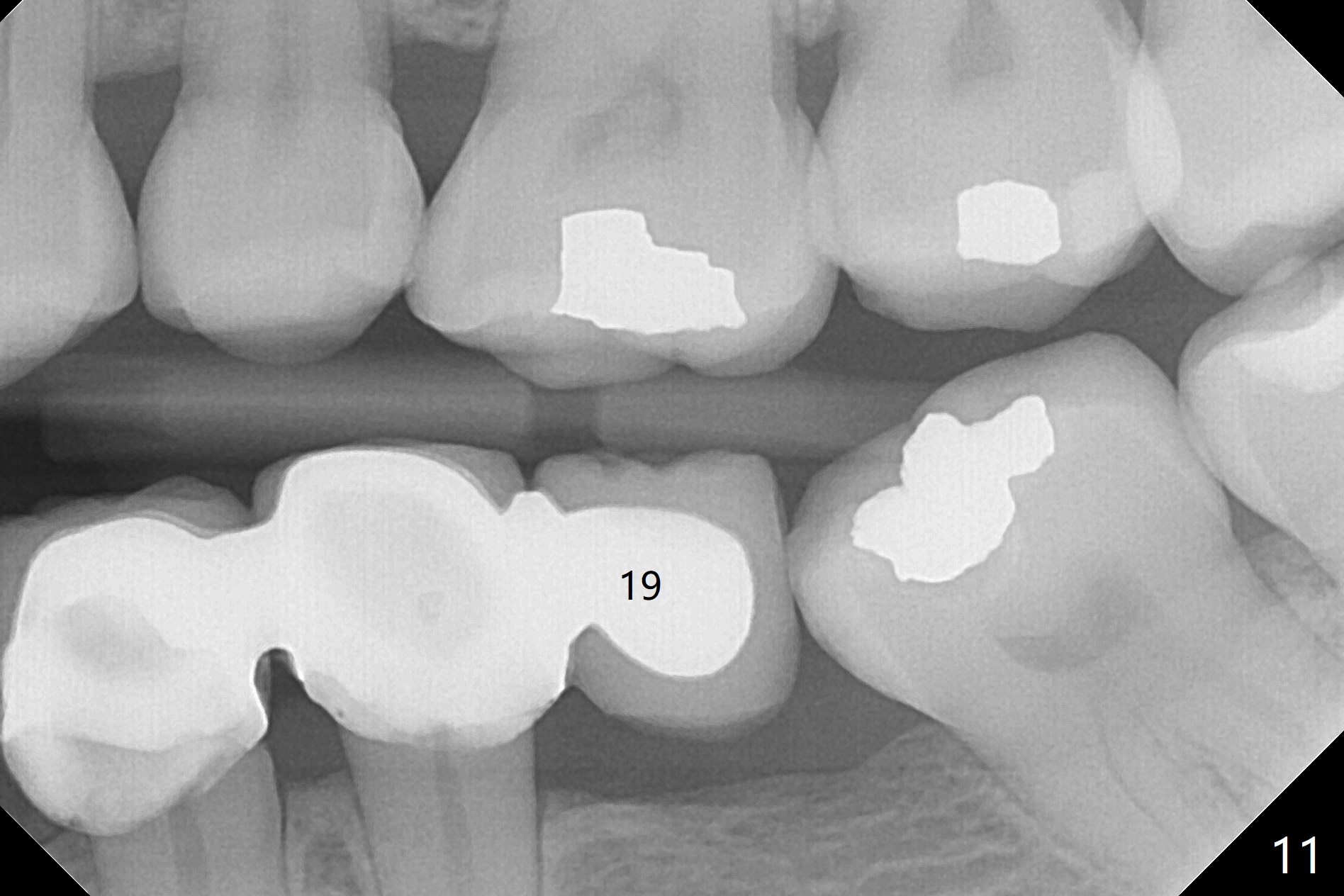
The patient returns for final restoration 3 months postop; bone resorption around the 1-piece implant is minimal (Fig.7). The definitive restoration is also splinted. The latter is further justified when the implant at #30 is found to be distal prior to cementation (Fig.8 *). It appears that implant spacing at the root level is more critical than parallelism, as compared to Fig.7. Let us improve this aspect. Bone loss around the implants remains minimal 7 months post cementation (Fig.9). It is the same 1 year 8 months post cementation (Fig.10), as compared to a cantilever FPD on the other side (Fig.11). The bone density around the implants at #30 and 31 increases 2 year 8 months post cementation (Fig.12).
Return to Lower Molar Immediate Implant,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 11/06/2015, last revision 10/20/2018