

|
|
|
|
|
|
|
|
|
|
|
|
|
|
Even Edentulous Spaces
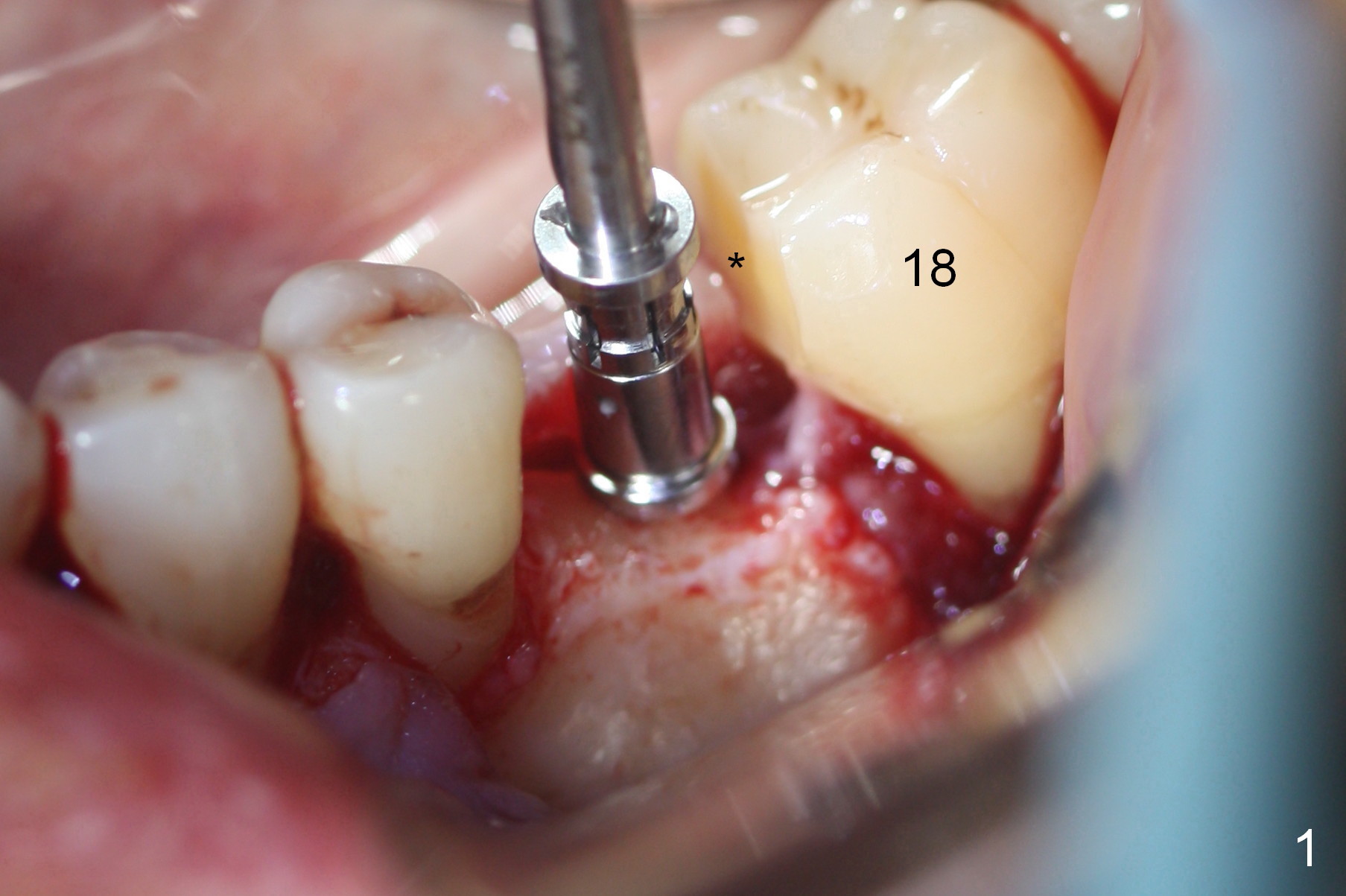
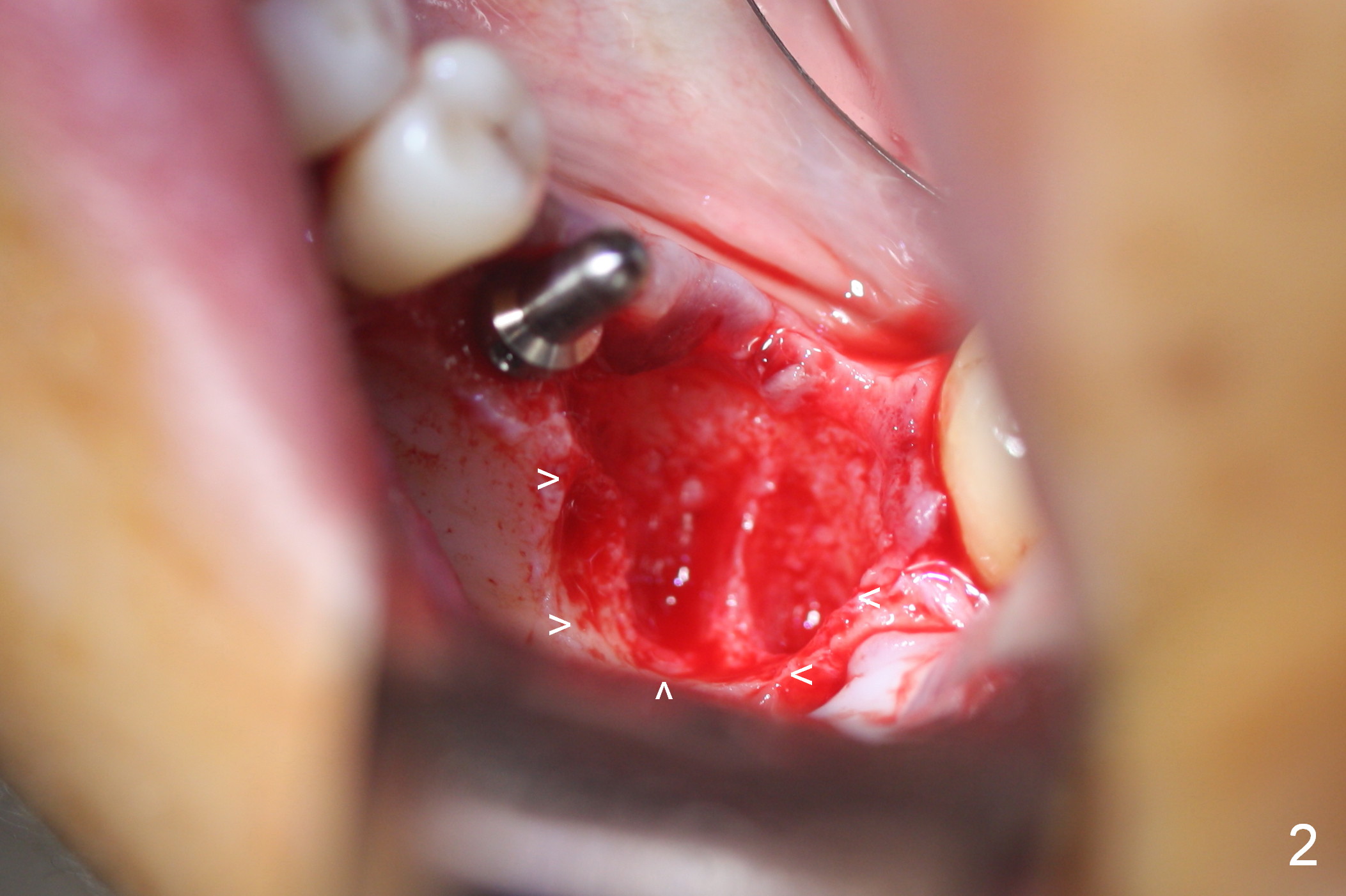
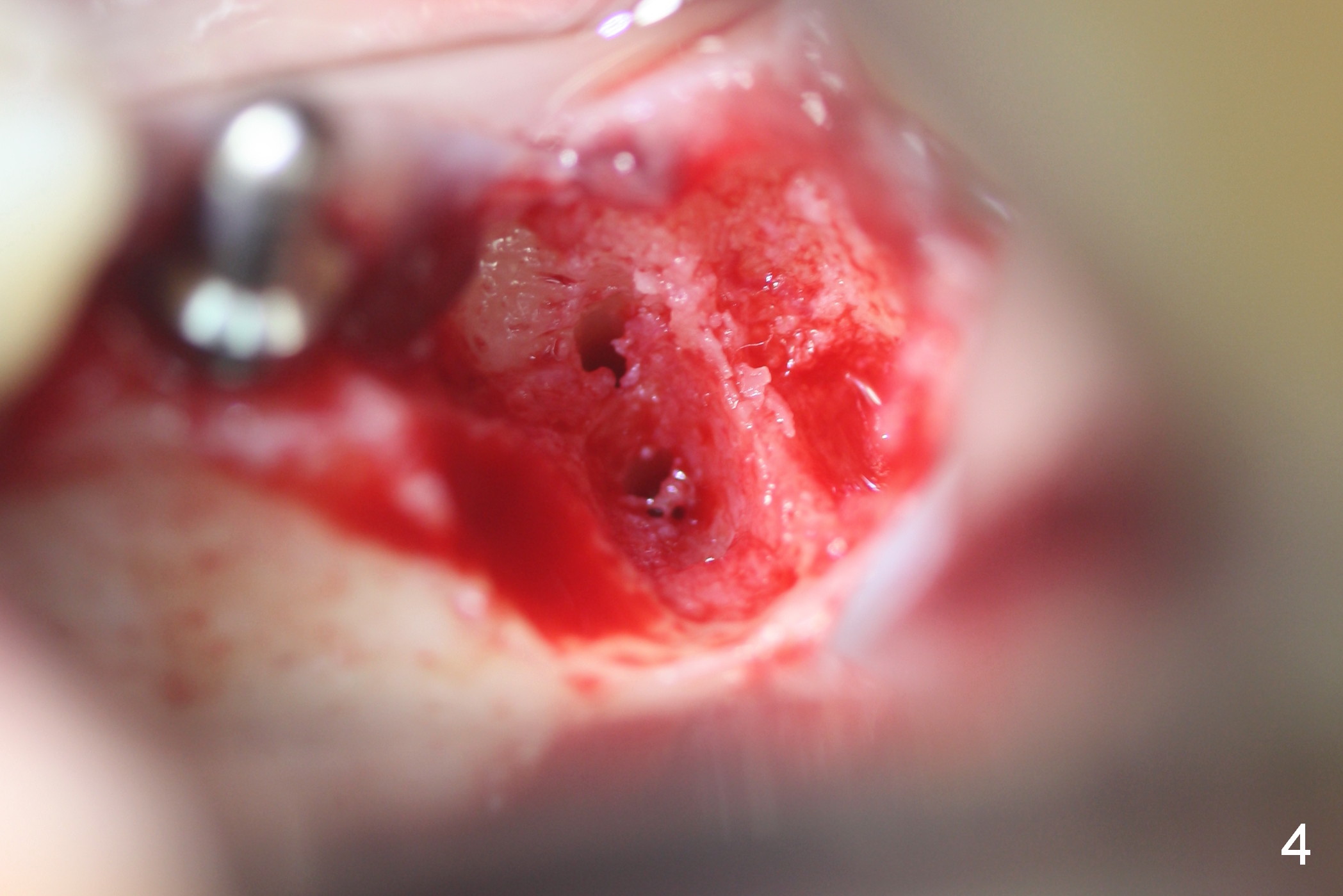
Since the tooth #18 has severely shifted and tilted mesially, the 2 edentulous spaces (#18 to be extracted) are evened by trimming the mesial surface of the tooth #18 (Fig.1 *) prior to osteotomy at #19. The axis of the osteotomy of #19 is parallel to the long axis of the mesial tooth, i.e., #20 (Fig.1-3). The advantage of non-flapless approach for immediate implant is better visualization of the buccal defect (Fig.2 arrowheads), precise positioning of osteotomy (Fig.4) and secure placement of bone graft (Fig.7-9*) and membrane after implant placement.
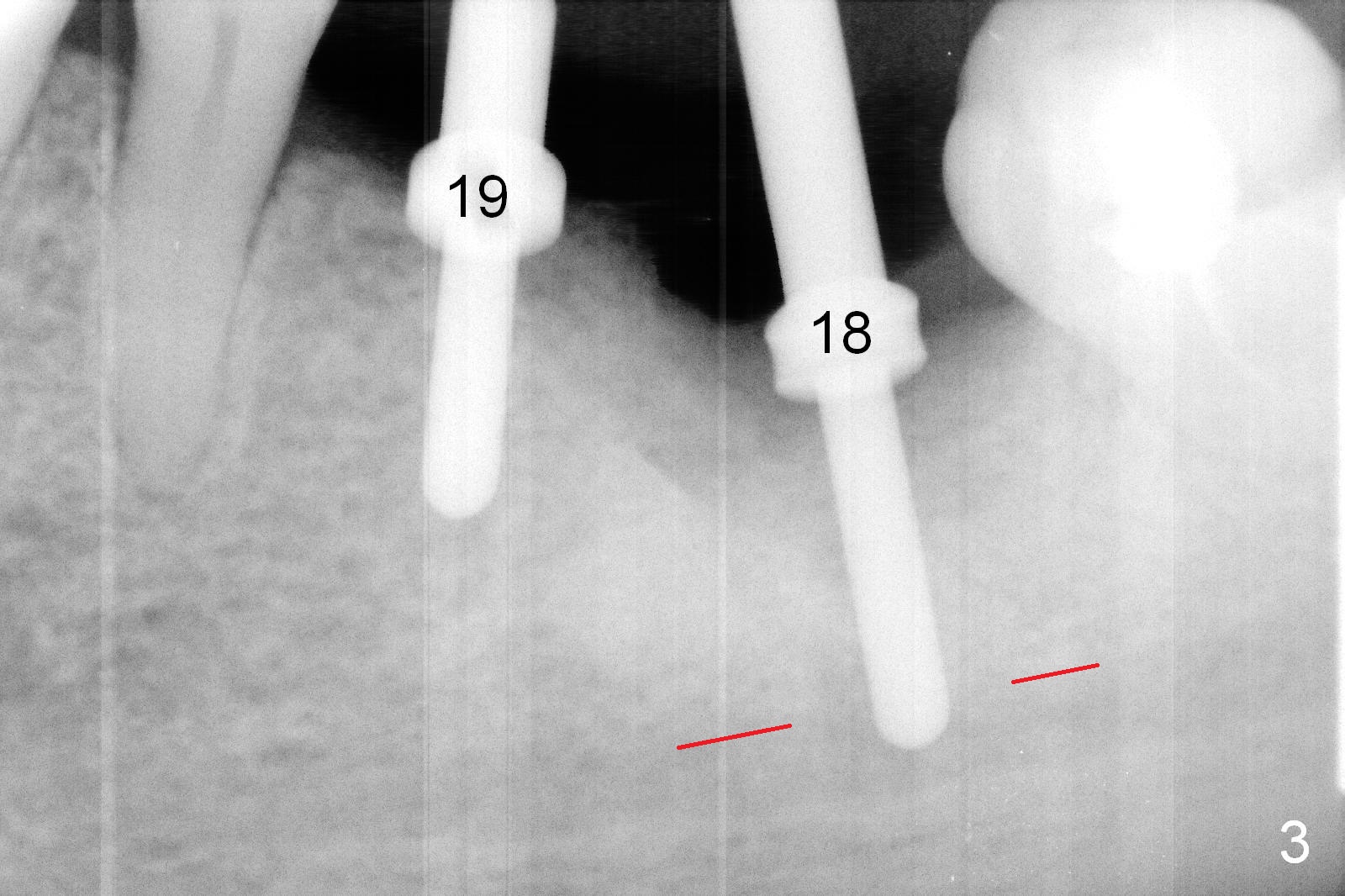
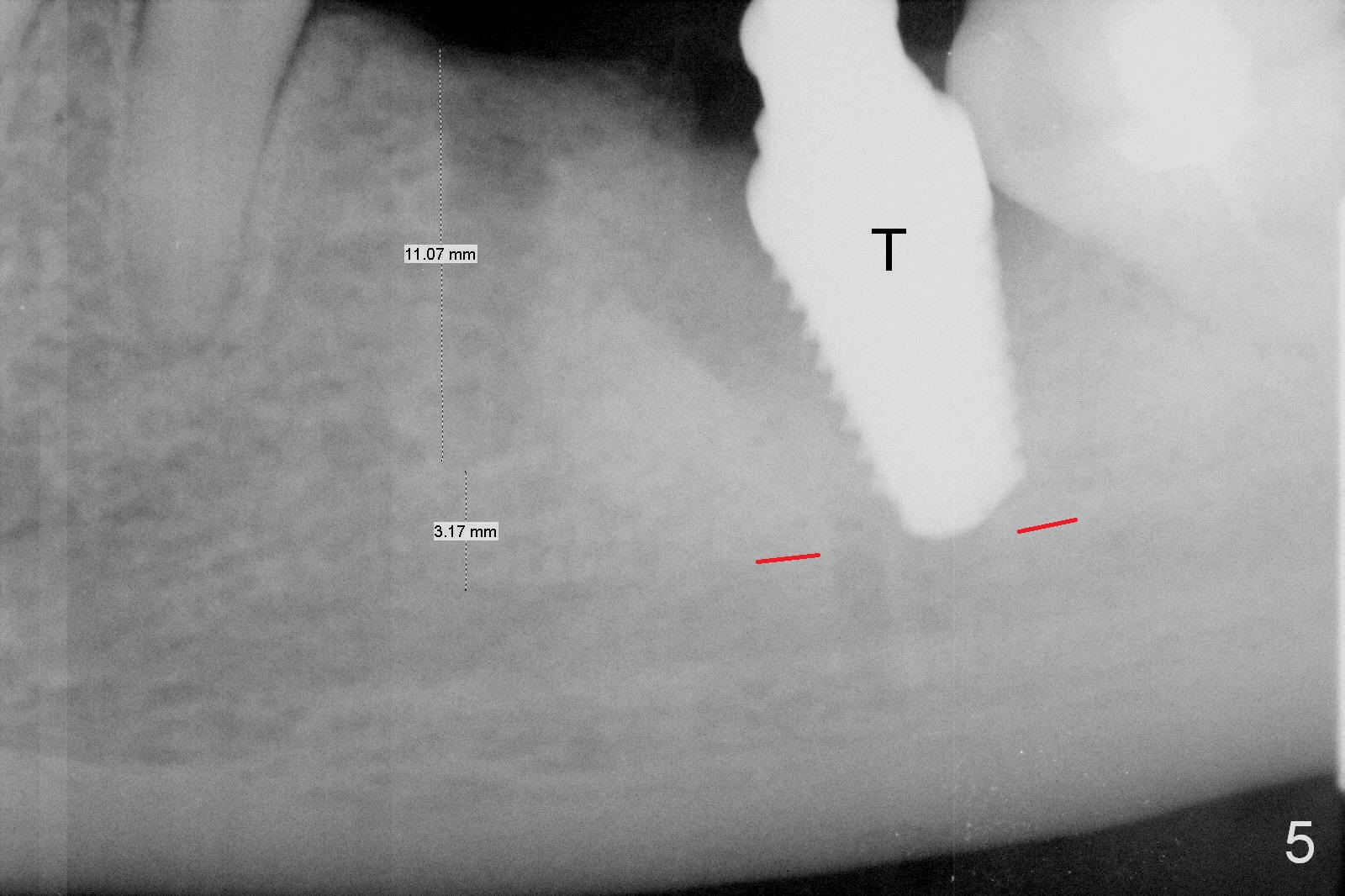
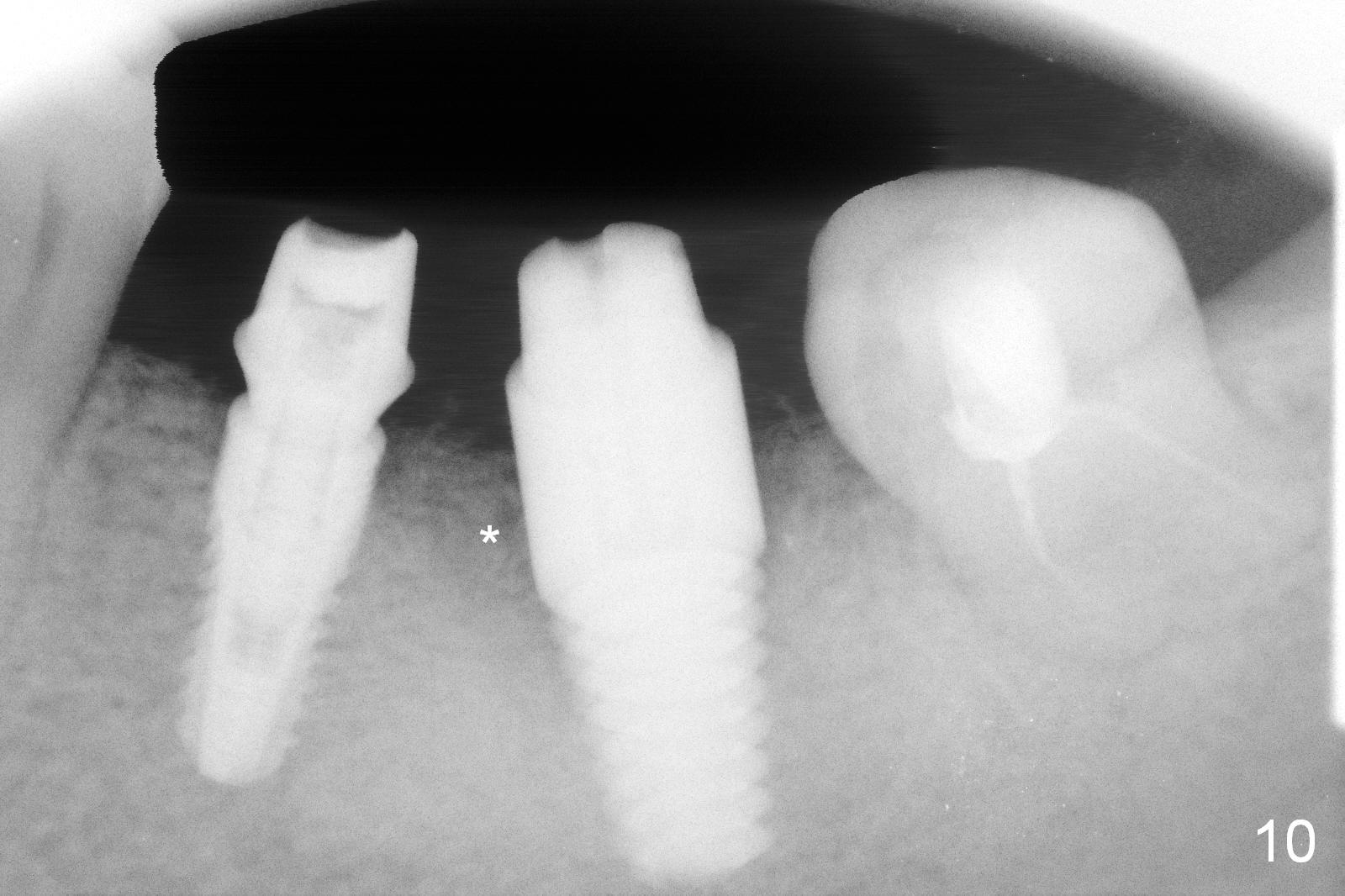
It is difficult to use Sinus Master Kit stoppers for osteotomy in the bottom of the narrow concave mesial socket at #18 (Fig.2,4). The depth control is more or less dependent on vision: stoppers against the mesial crest of the mesial socket. The initial osteotomy appears to invade the Inferior Alveolar Canal (Fig.3), although there is no clinical sign of canal invasion (no brisk hemorrhage from the bottom of the osteotomy, nor severe pain with infiltration anesthesia). After reducing the depth, the patient tolerates further osteotomy until 6x14 mm tap achieve primary stability (Fig.5 T). In fact the patient cannot bear pain associated with osteotomy at #19. Block anesthesia is administered for the remaining osteotomy and implant placement (Fig.6). As routine, splinted immediate provisional is fabricated for wound protection. The patient returns for impression 4 months postop; bone density in the mesial socket of #18 appears to increase (Fig.10 *).
There is mild tenderness at #18 when the splinted provisional is being removed. The latter has to be sectioned prior to its removal. The gingiva appears normal at #18 and 19. The definitive restoration is delivered. The repair of the incisal fracture at #9 commences.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 02/18/2016, last revision 07/10/2016