



|
|
|
|
|
|
|
|
|
|
|
Delayed Implant is Safer than Immediate One for Lower 2nd Molar
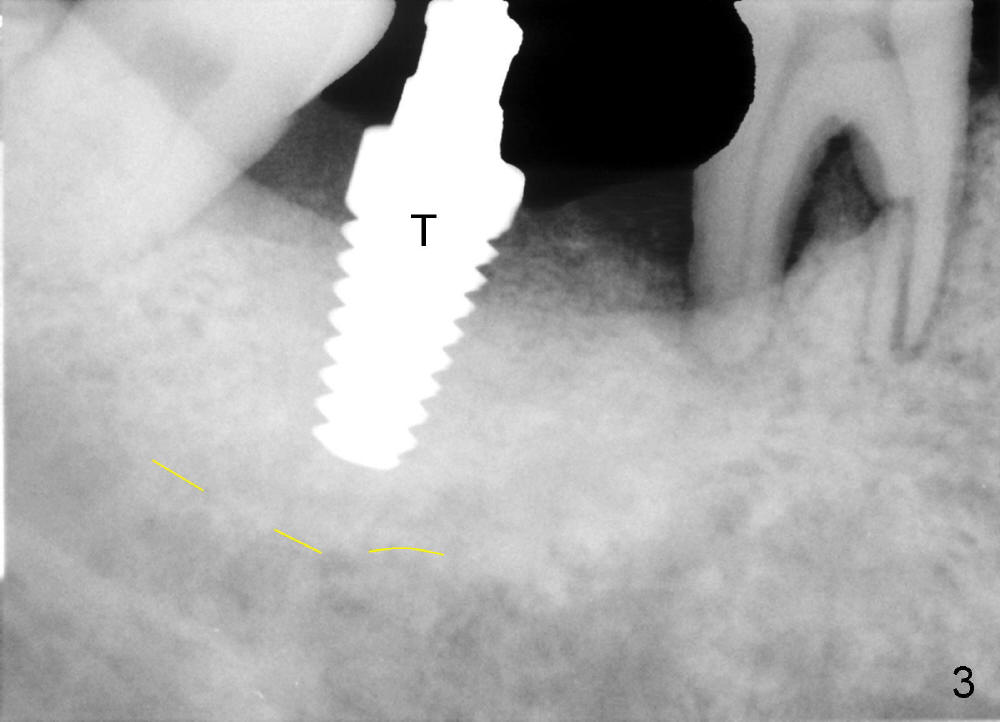
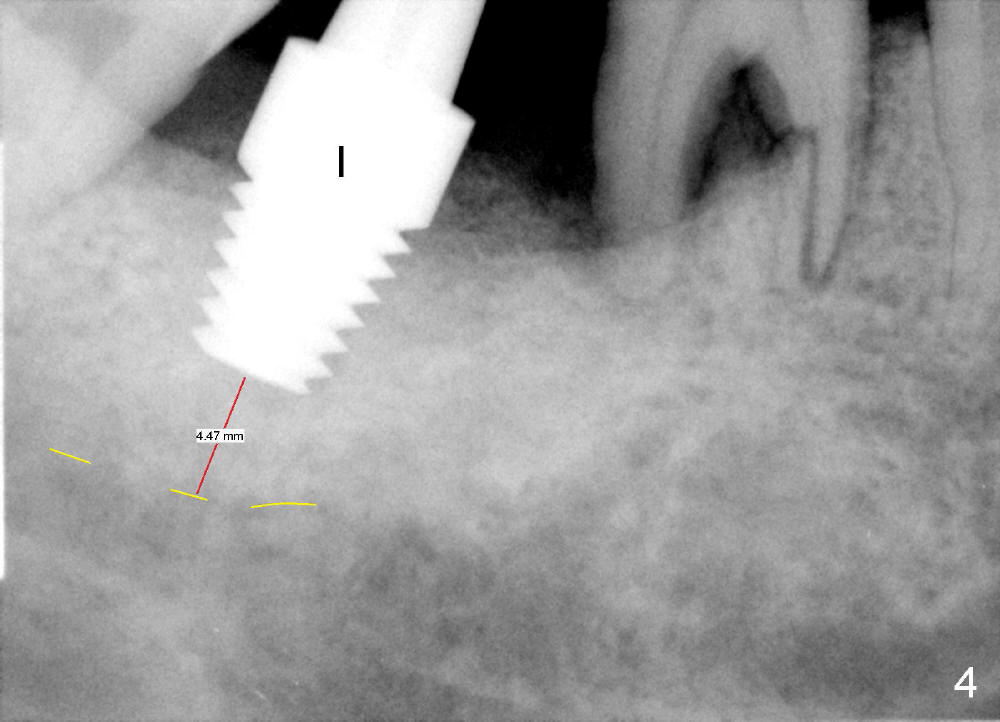
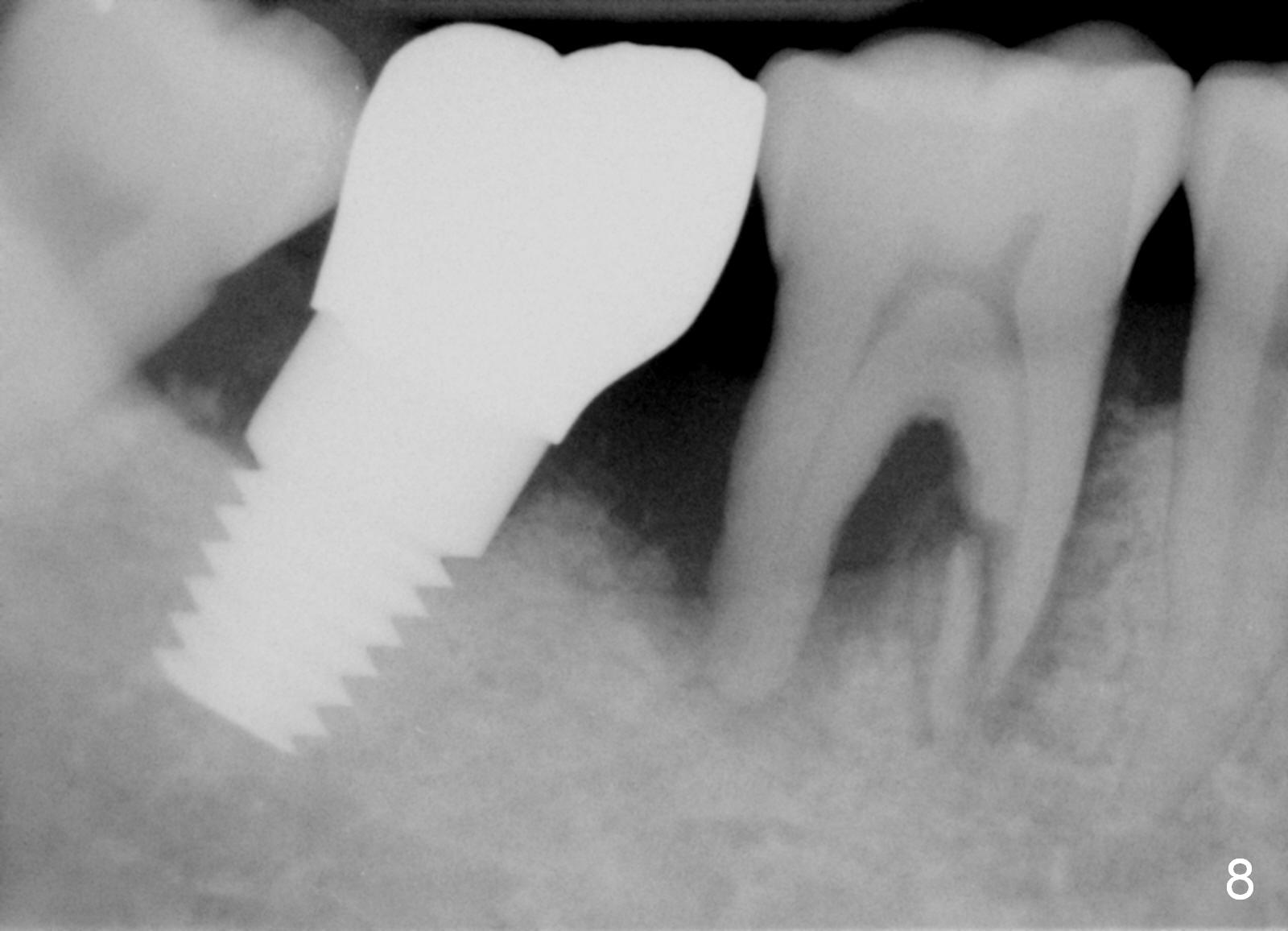
Luckily the patient returns for #31 implantation 4 months post socket preservation. Bone forms in the alveolus and above (Fig.1 black and white arrowheads, respectively). A 6 mm tissue punch is used to open the wound (Fig.2). Osteotomy forms using bone expanders, reamers and taps (Fig.3: 6x14 mm tap). Without infection, local anesthesia is more easily achieved than immediate implant when infection exists. The depth is controlled more readily with delayed implantation. Following adjustment of trajectory, a 7x11 mm implant is placed with insertion torque 60 Ncm (Fig.4 I). Fig.5 shows that the implant obliterates the wound; an abutment (A) is placed to retain perio dressing. With formation of new bone from socket preservation, insertion torque seems to be more easily obtained with the short implant. There is no space to re-use the harvested bone (Fig.6). The implant remains stable postop. Apparent new bone is forming toward the distal coronal threads 5 months postop (Fig.7). The bone around the implant remains stable 17 months post cementation (Fig.8), although there is an episode infection at the neighboring tooth (#30). The patient is more eager to have implants for the maxilla, since the flipper has lost. After implant placement at #7, the pain at #30 becomes more severe.
Return to Lower Molar Immediate Implant
Xin Wei, DDS, PhD, MS 1st edition 10/02/2014, last revision 09/25/2016