
.jpg)
.jpg)


%20just%20removed%20from%20crown%20PA,%20oblique.jpg)
%20just%20removed%20from%20crown%20BW,%20gap.jpg)
%20trimmed%20before%20sensor%201.jpg)
,%20no%20angulation.jpg)

|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
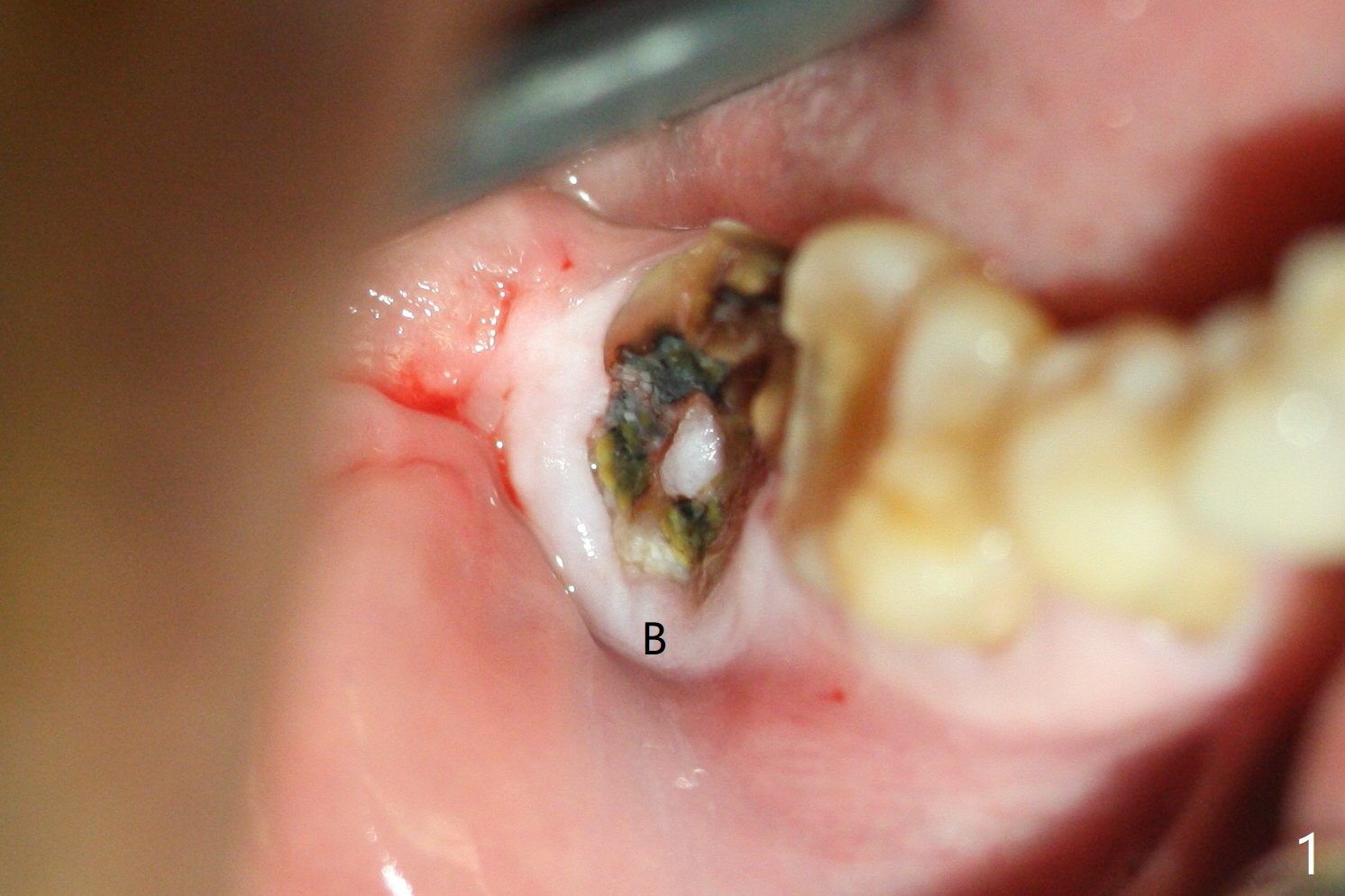
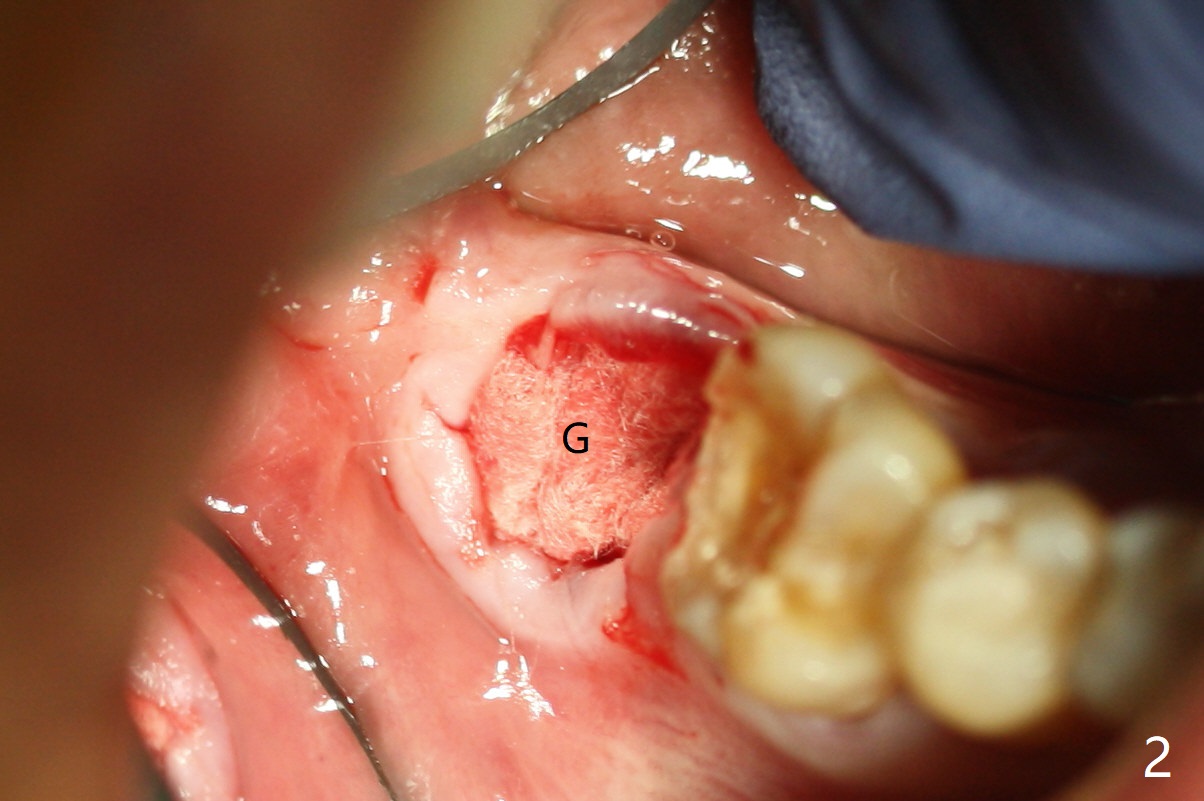
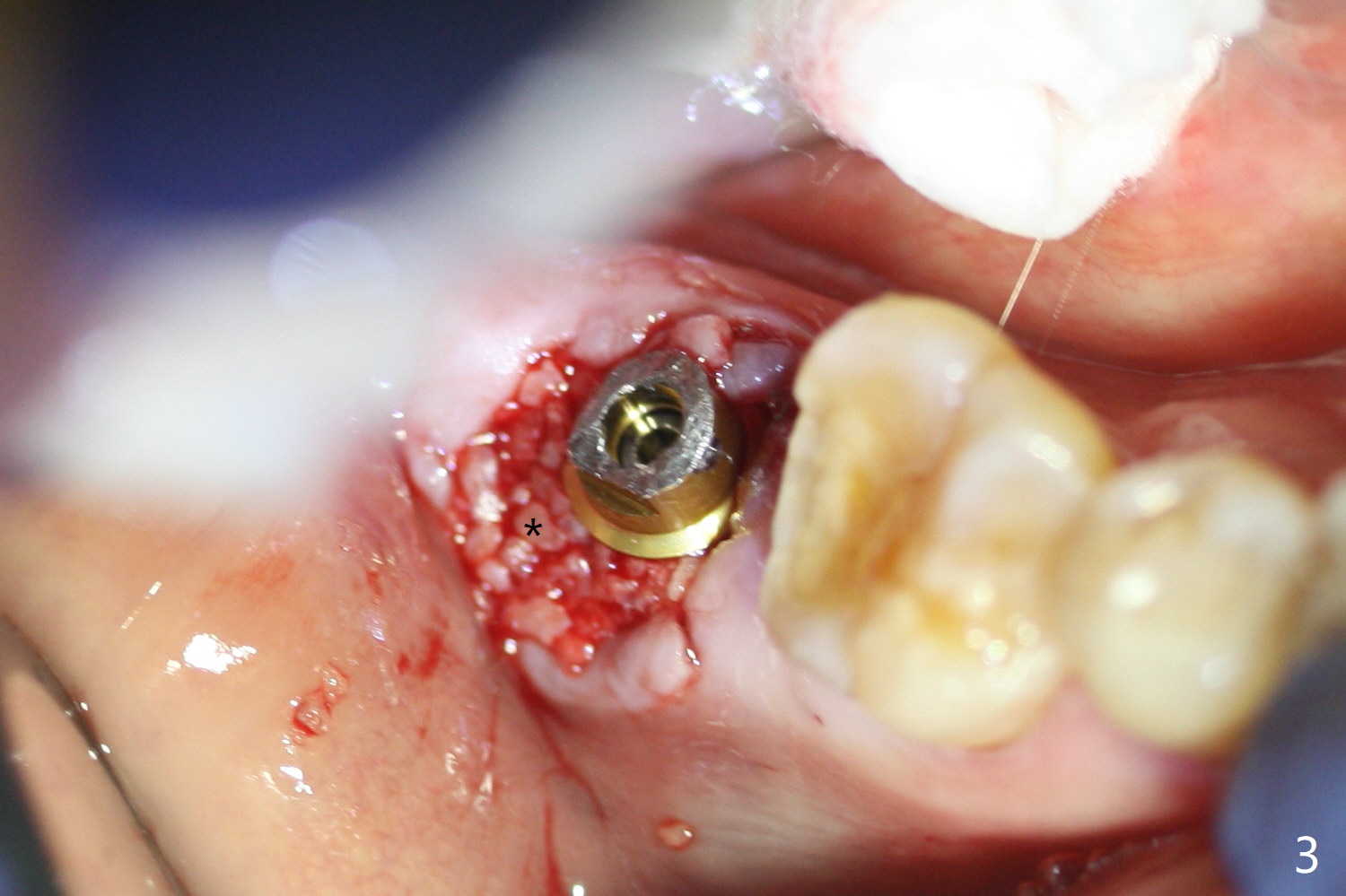
Guided Immediate Implant Associated with Opposing Tooth Supraeruption
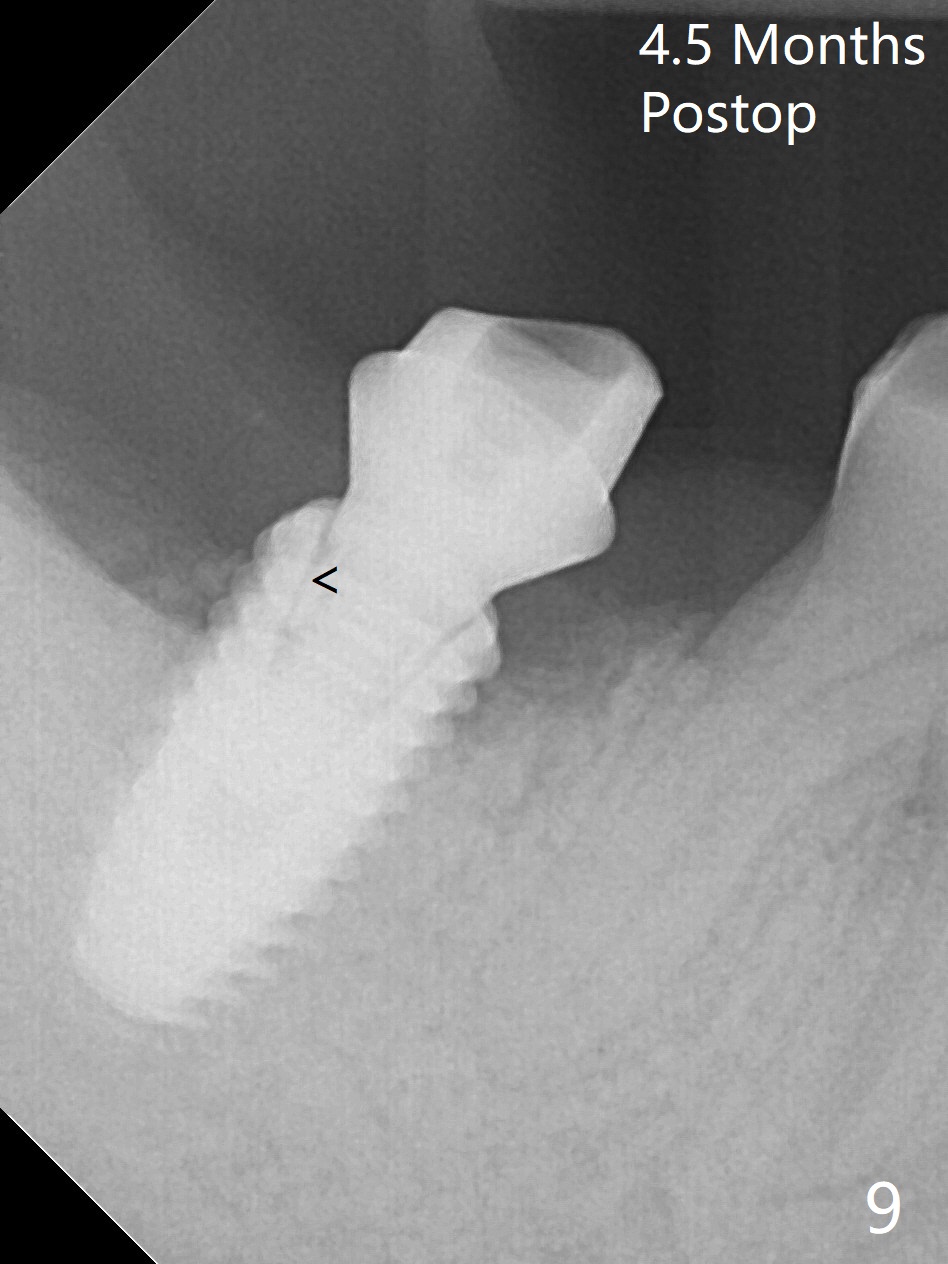
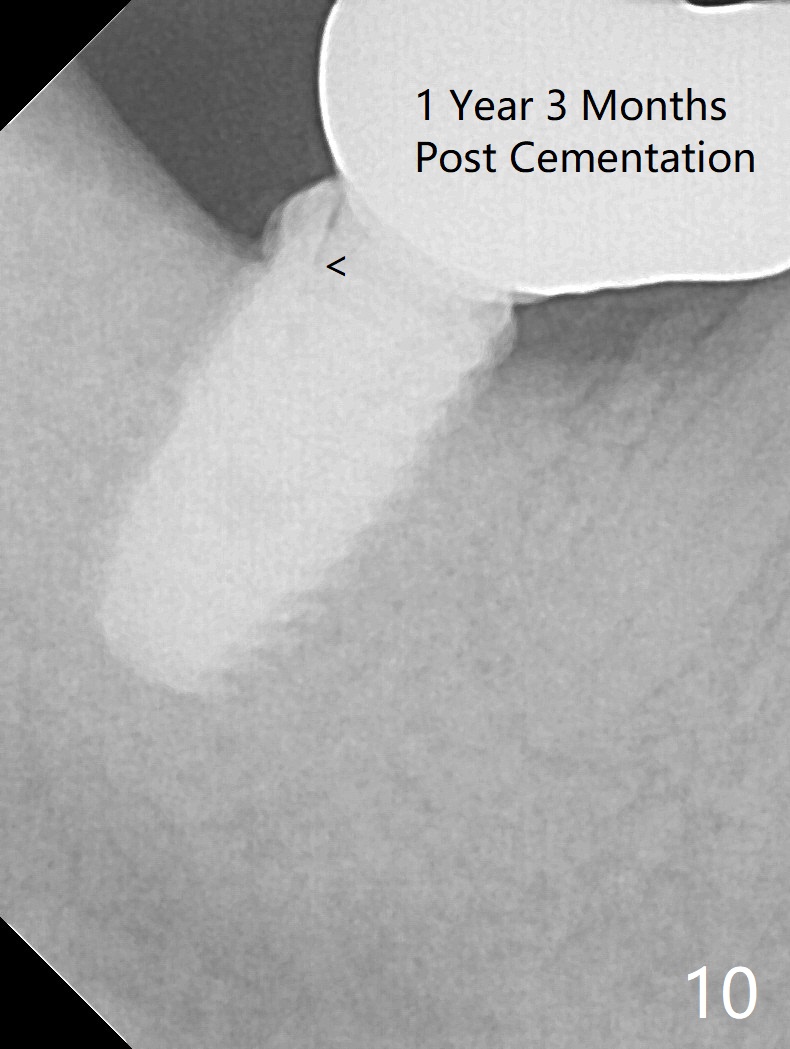
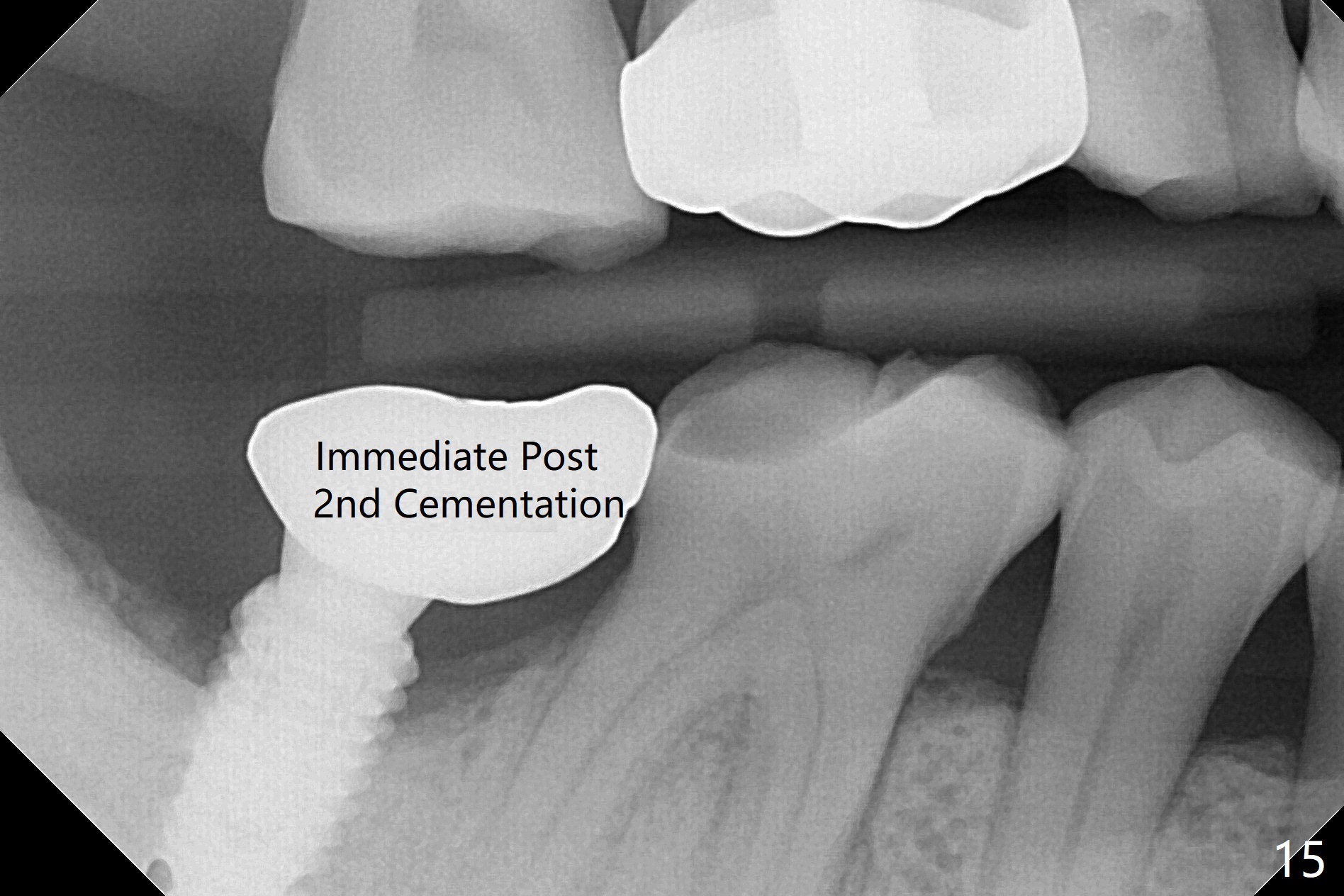
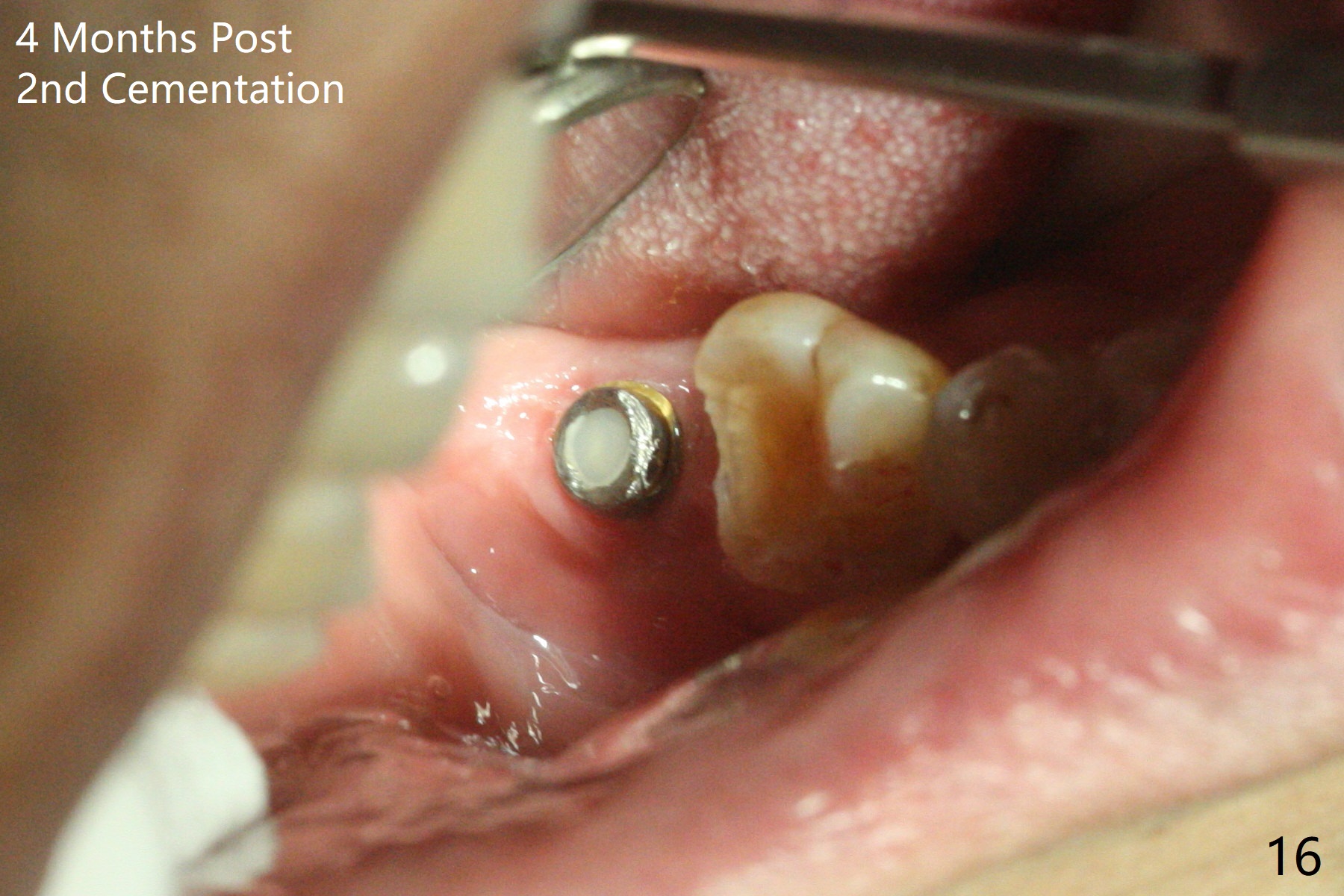
The residual roots of the tooth #31 are lower buccal (Fig.1 B), which in fact is molded and worn by the supraerupted tooth #2. When the tooth is extracted (Fig.2) and an implant, abutment (Fig.3 gold colored) and allograft (*) are placed, the abutment has to be trimmed. An atypical immediate provisional is fabricated by spreading setting acrylic over the abutment and bone graft (Fig.4 P) with occlusal equilibrium. Advantages of the guided surgery are good position (Fig.3 buccolingual), trajectory and depth (Fig.5,6) of the implant. The buccodistally exposed implant threads are packed with allograft in sufficient amount (Fig.3,5,6 *). The atypical immediate provisional breaks down and dislodges 3 weeks postop (Fig.7). In fact the implant plateau is exposed buccally. A monojet is given to the patient for self cleansing. He is instructed to return in 3 weeks. The exposed implant threads are covered 1.5 months postop (Fig.8). Incomplete abutment seating (Fig.9 <) was not noted until 1 year 3 month post cementation when the crown was mobile (Fig.10). A 6x3 mm healing abutment is placed. Three days later, the crown is sectioned and separated from the abutment. The latter returns to place; due to angulation associated with PA, the gap between the implant and abutment is indistinct (Fig.11). Bitewing is taken; the gap exists (Fig.12 <). The abutment seems to be seated deep; there is apparently soft tissue interference. A 5.2x4(2) mm abutment remains incompletely seated (Fig.13 >). A 5.2x4(3) mm one is completely seated (Fig.14 <). Zirconium crown with an access hole is cemented in the mouth. The crown and abutment is then removed for residual cement removal and reseated and torqued (Fig.15). Four months later, the Zirconium crown is fractured (Fig.16). Impression is retaken for high noble metal crown without access hole for strength (Fig.17).
Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), Trajectory, Ortho Cases, Weichat Xin Wei, DDS, PhD, MS 1st edition 01/13/2019, last revision 01/21/2021