

,%20prep,%20Vanilla.jpg)













mm.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
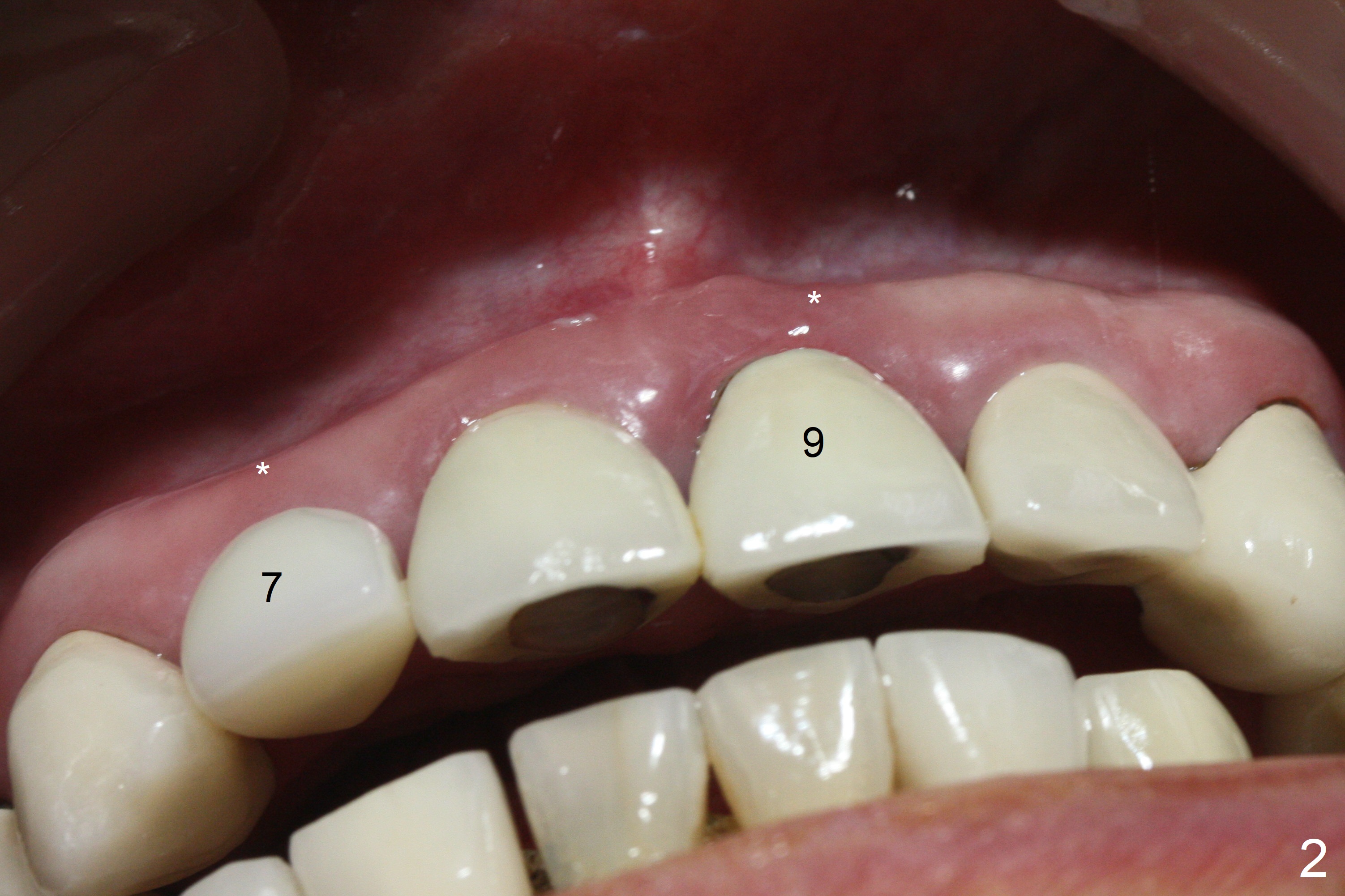
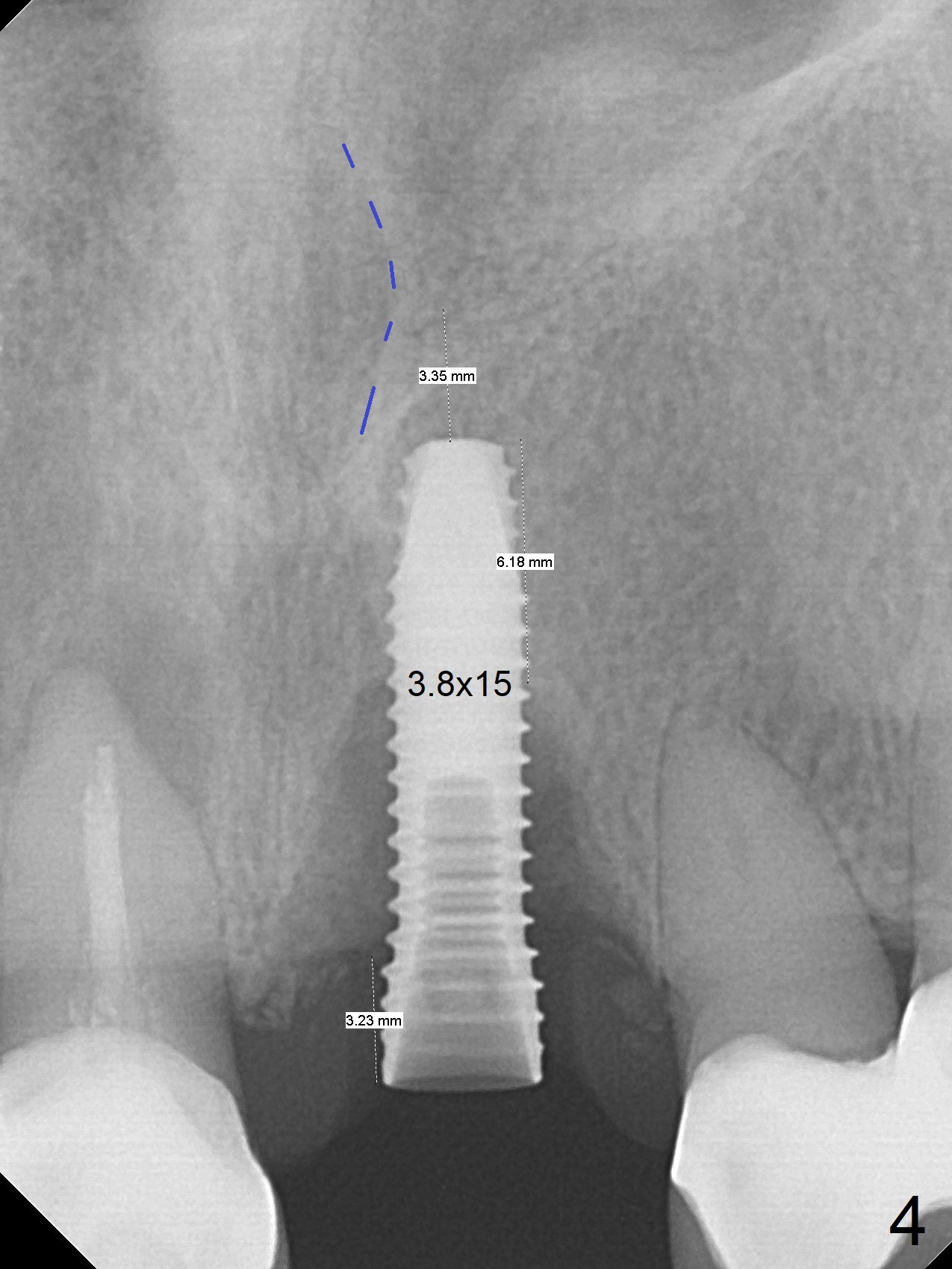
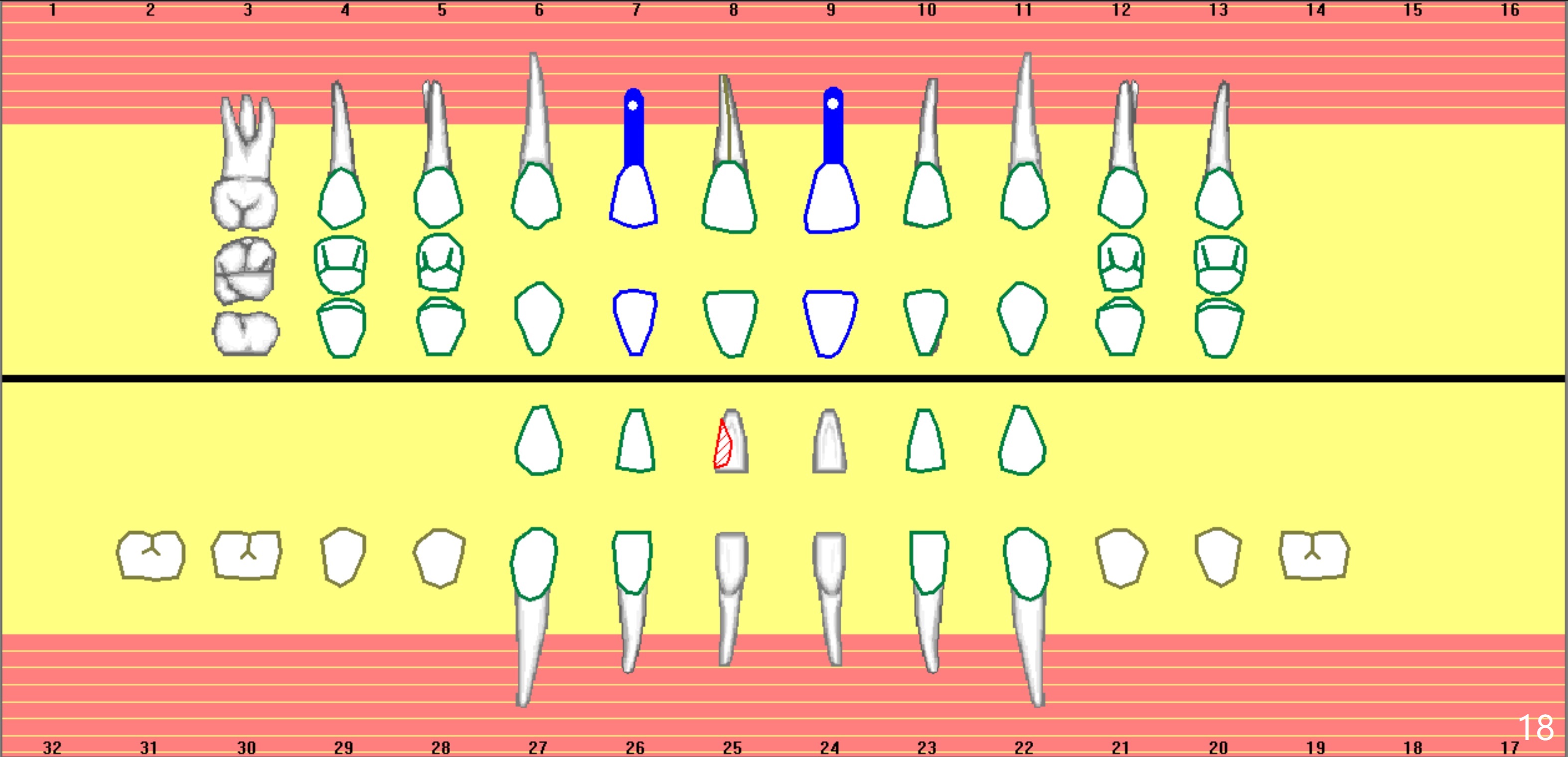
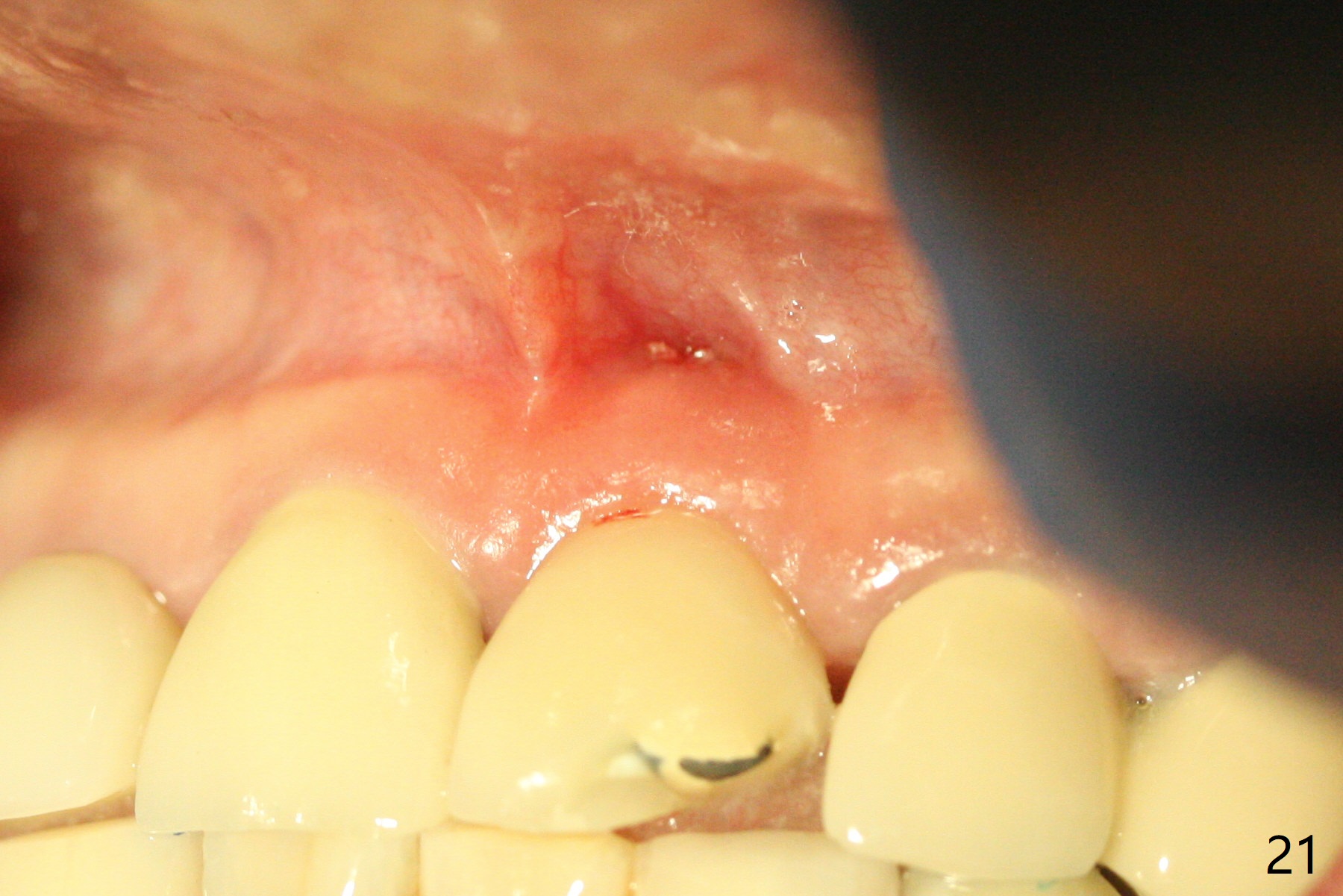
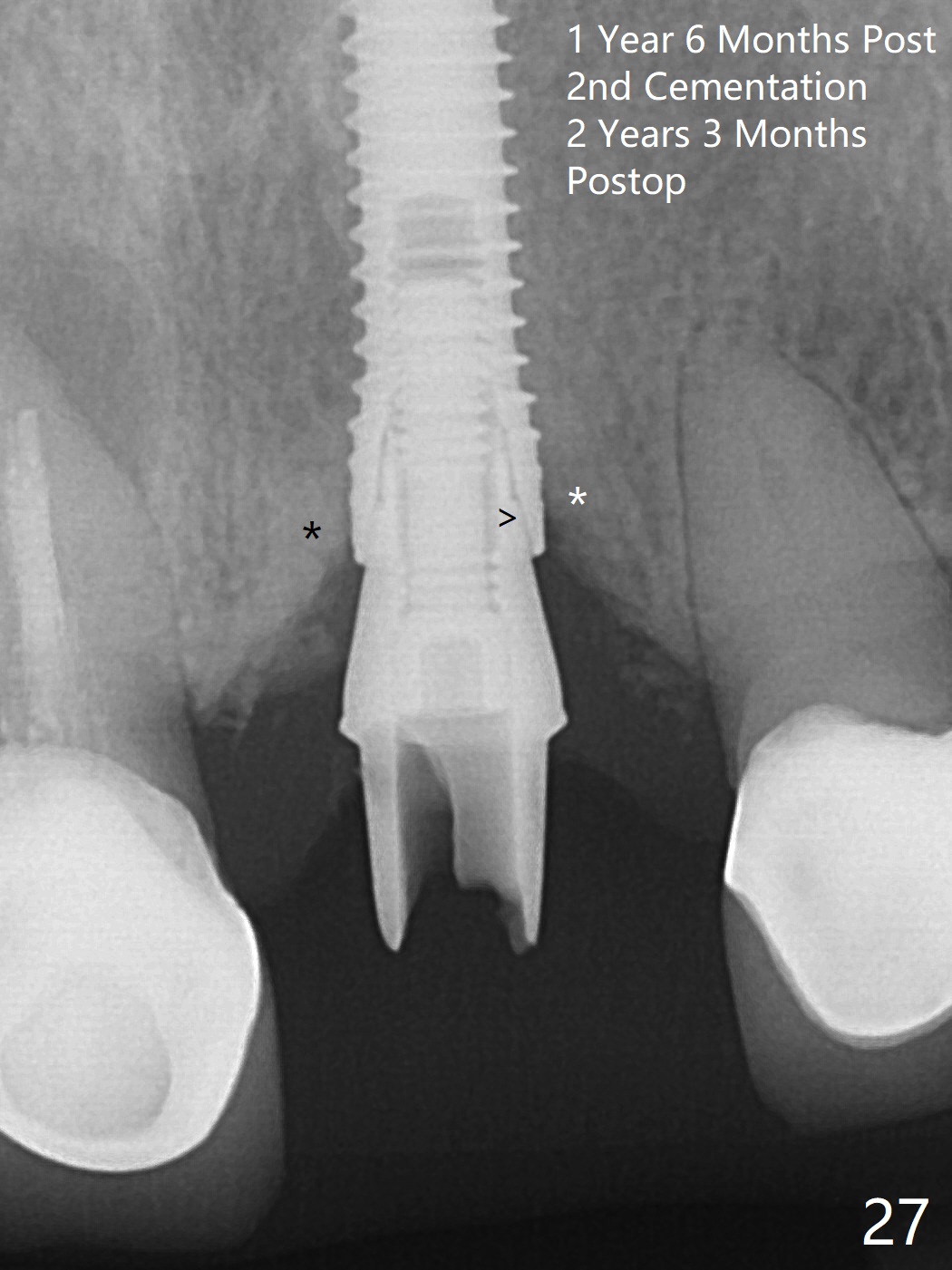
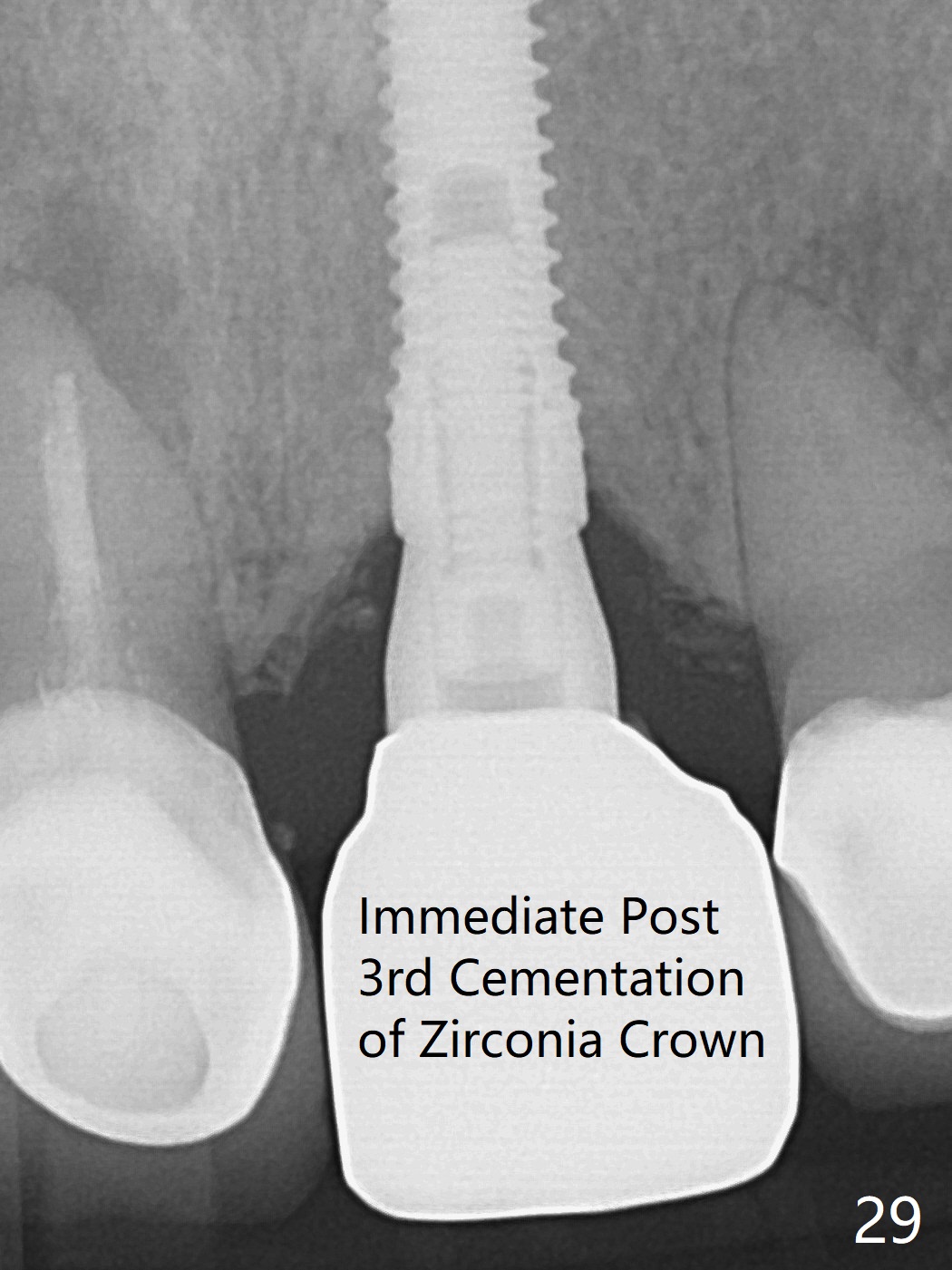
3.8x15 mm Implant with Proximity to
Nasal Floor
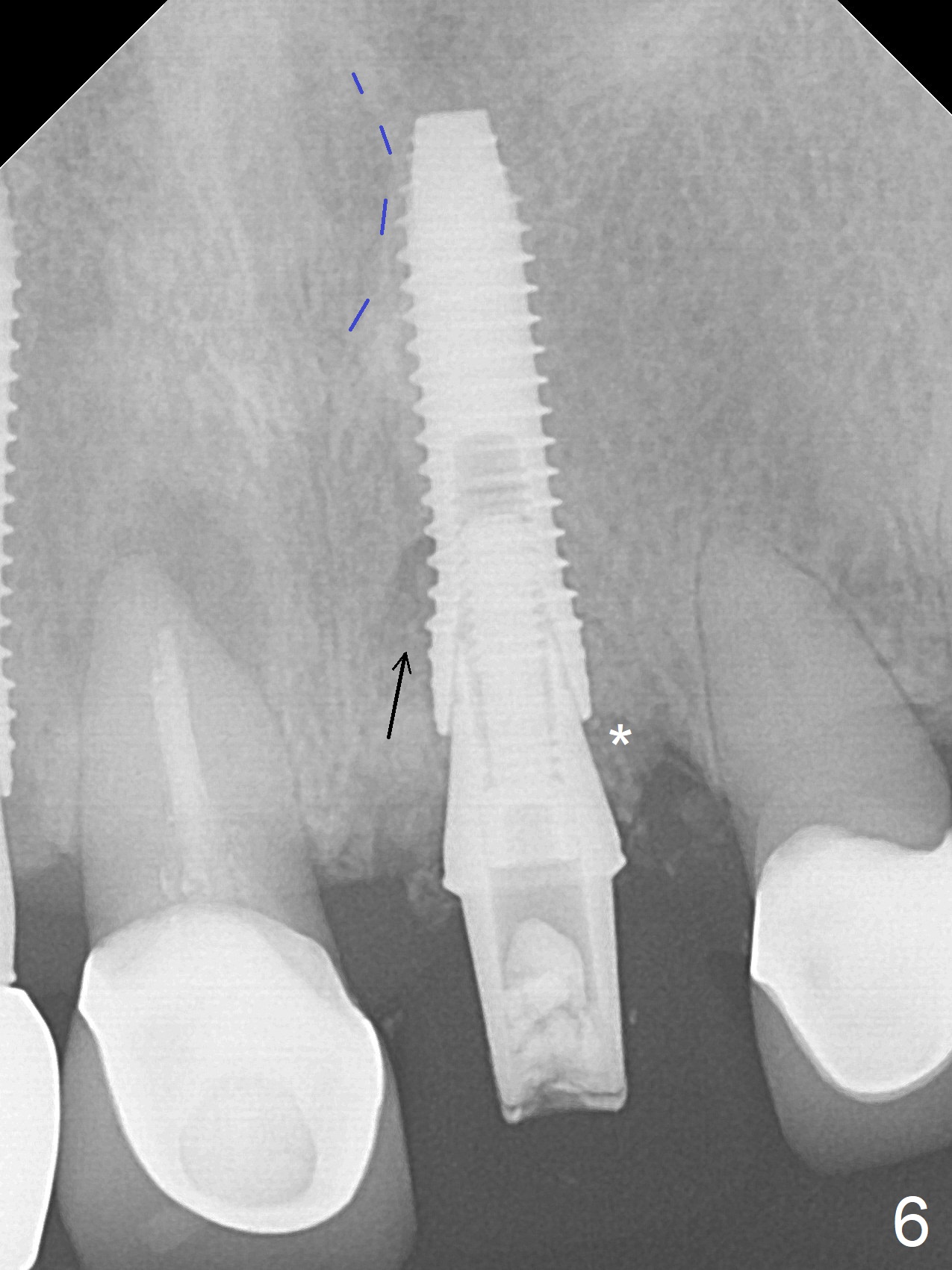
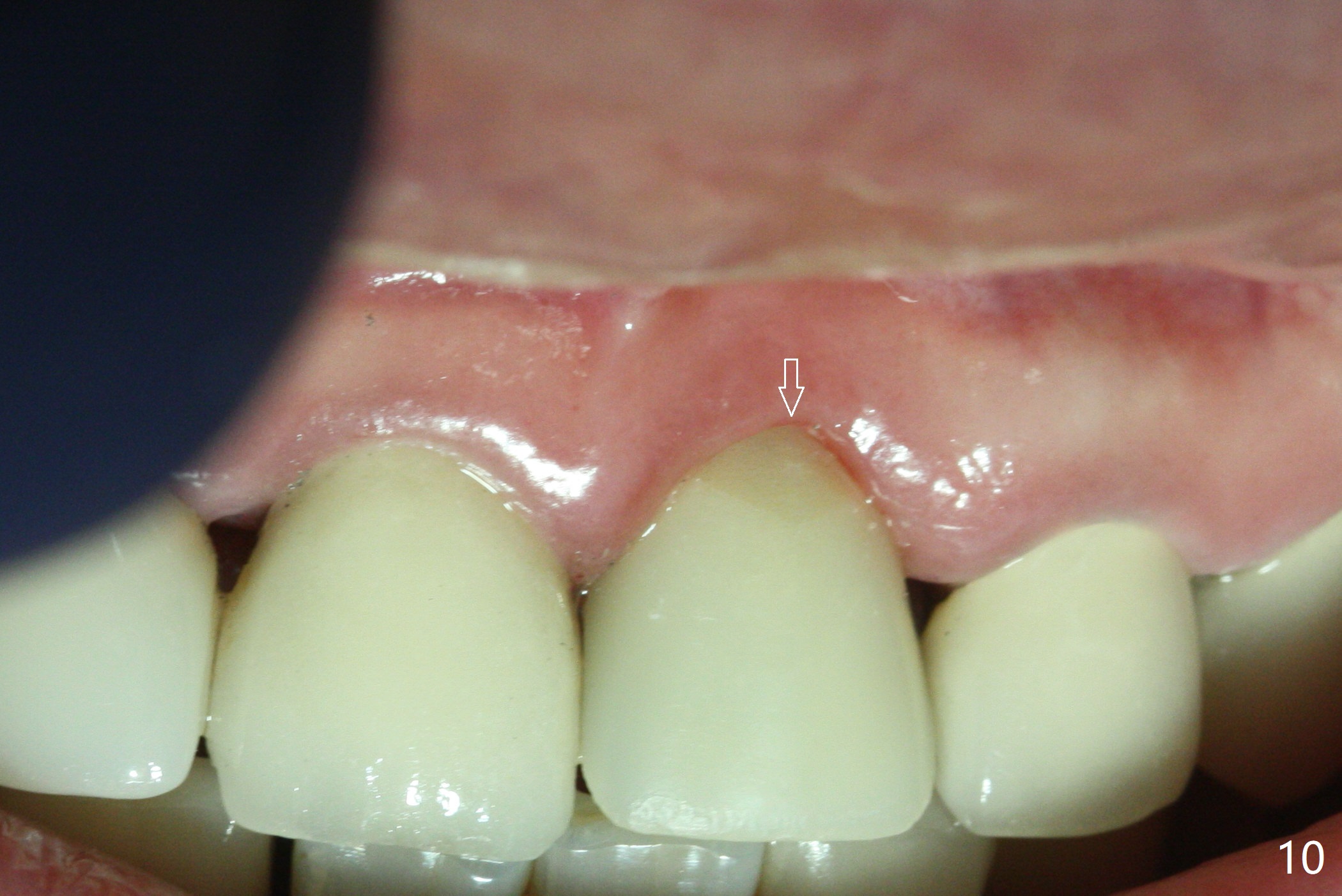
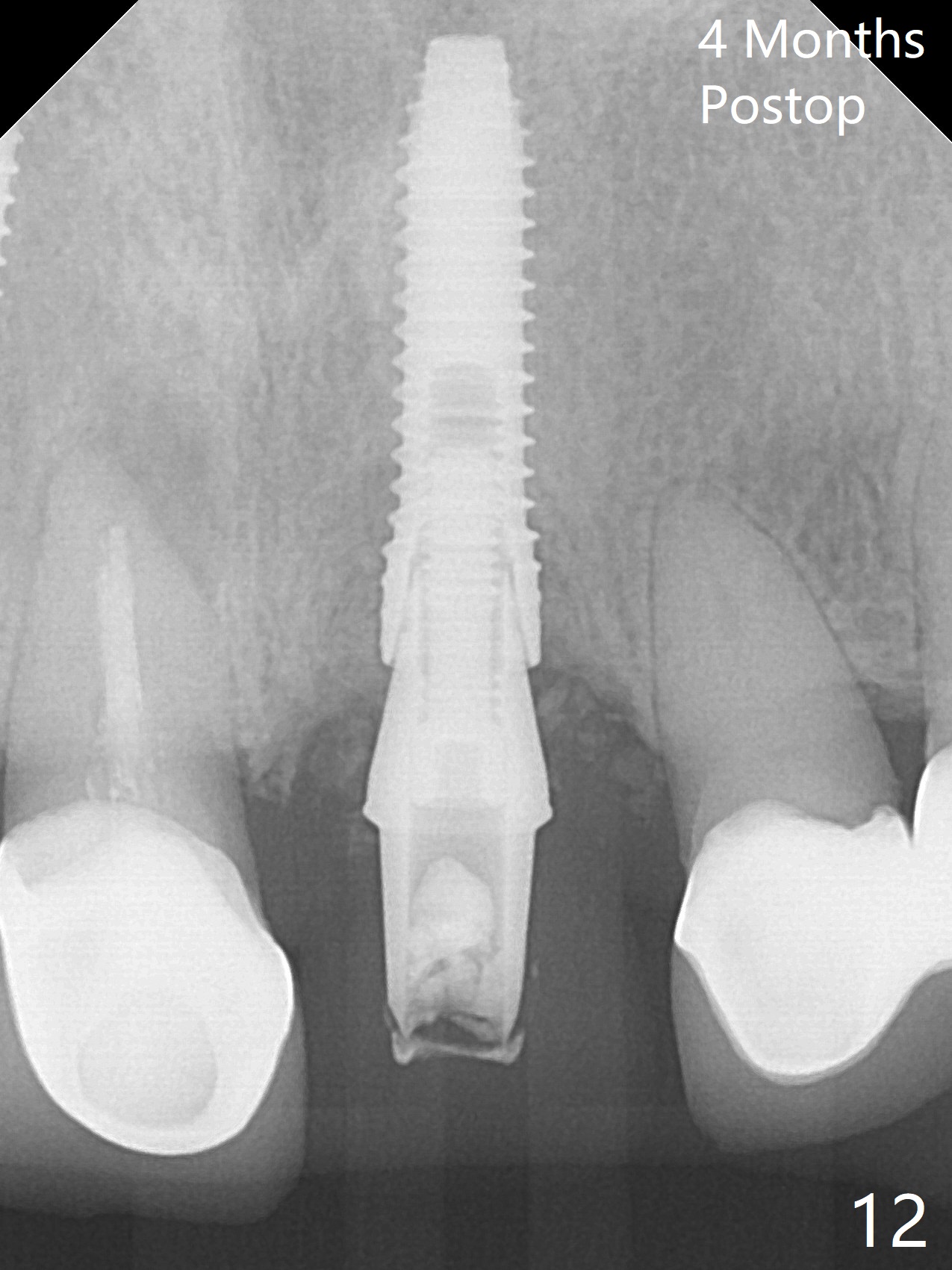
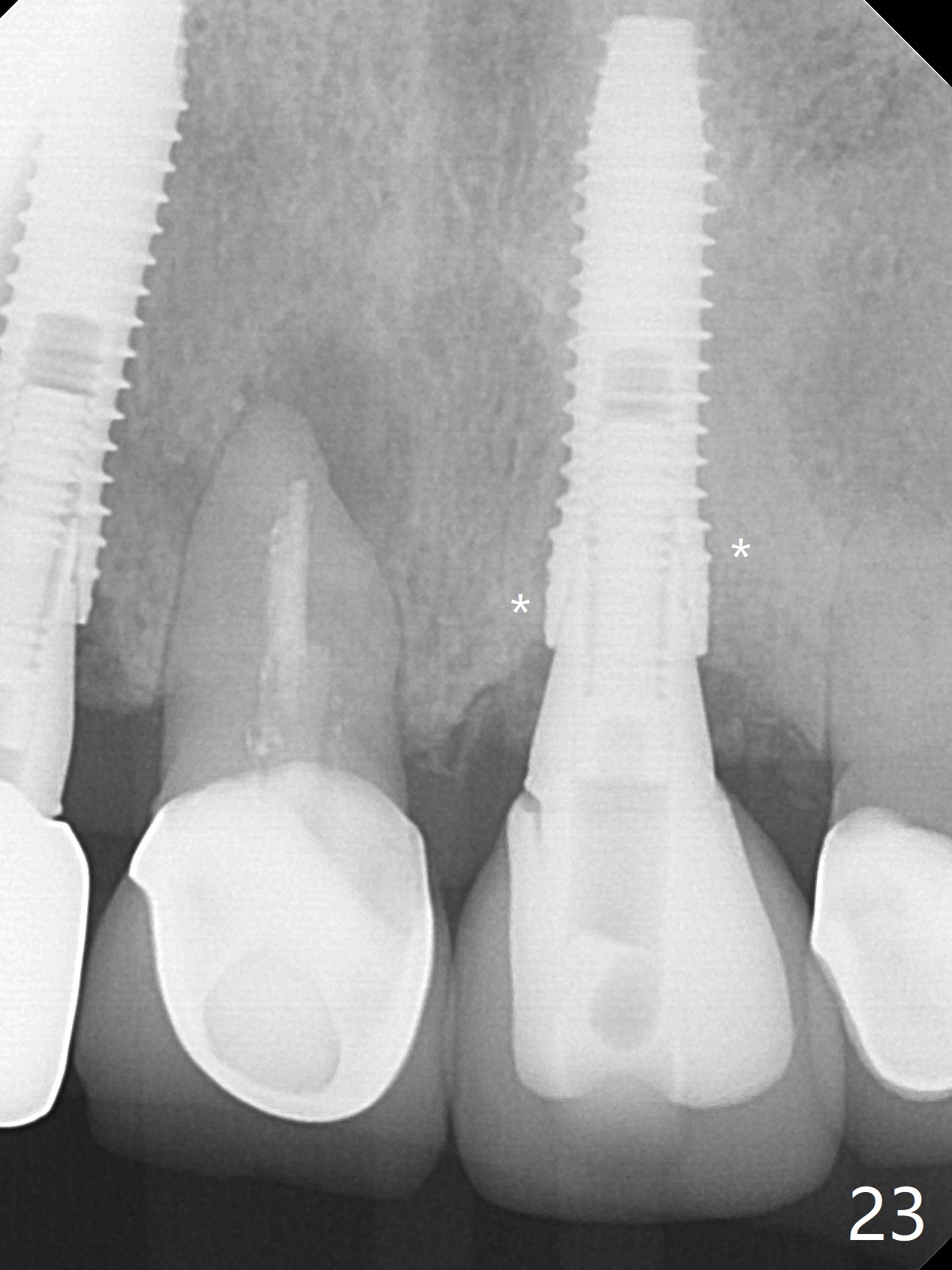
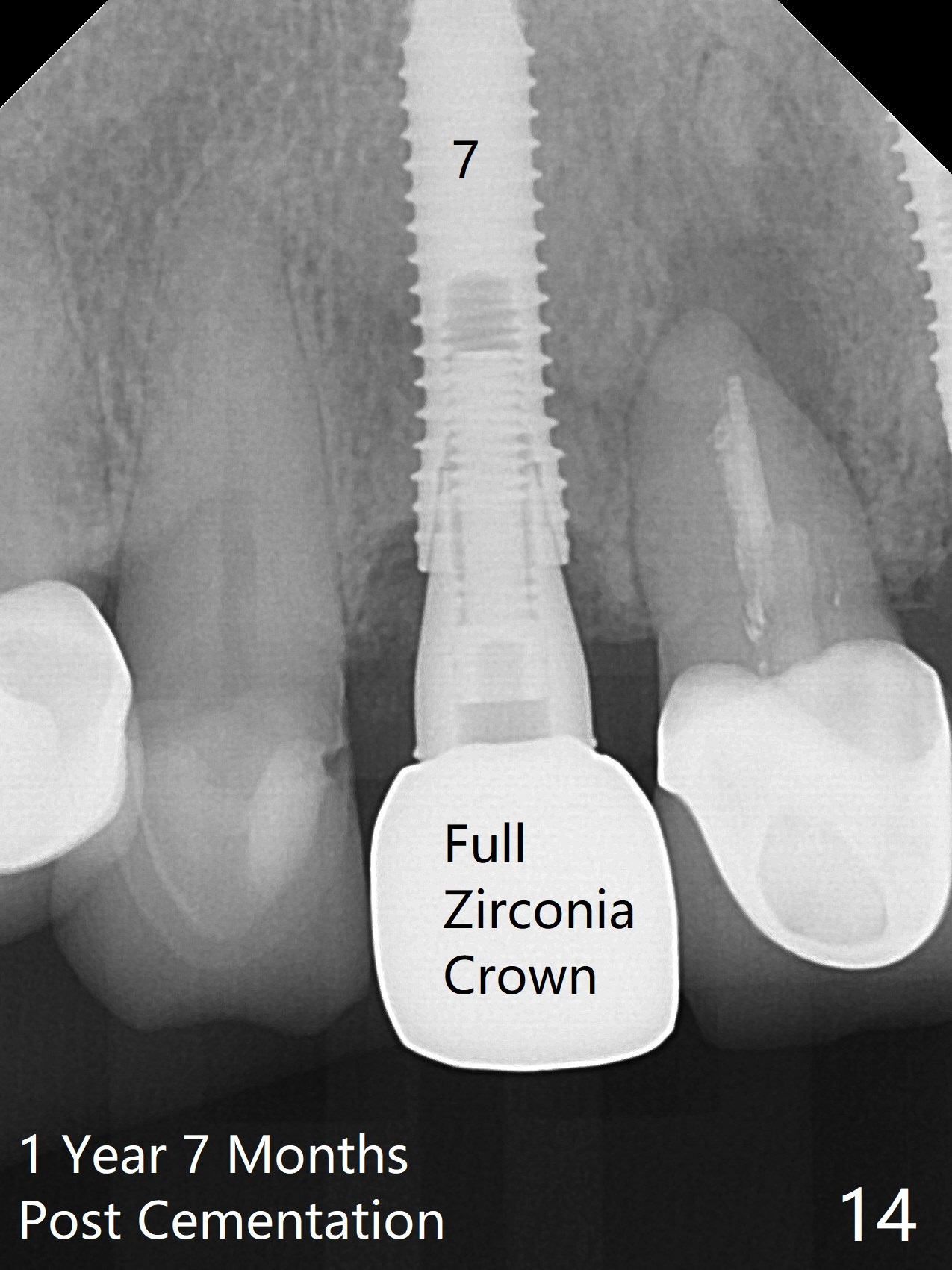
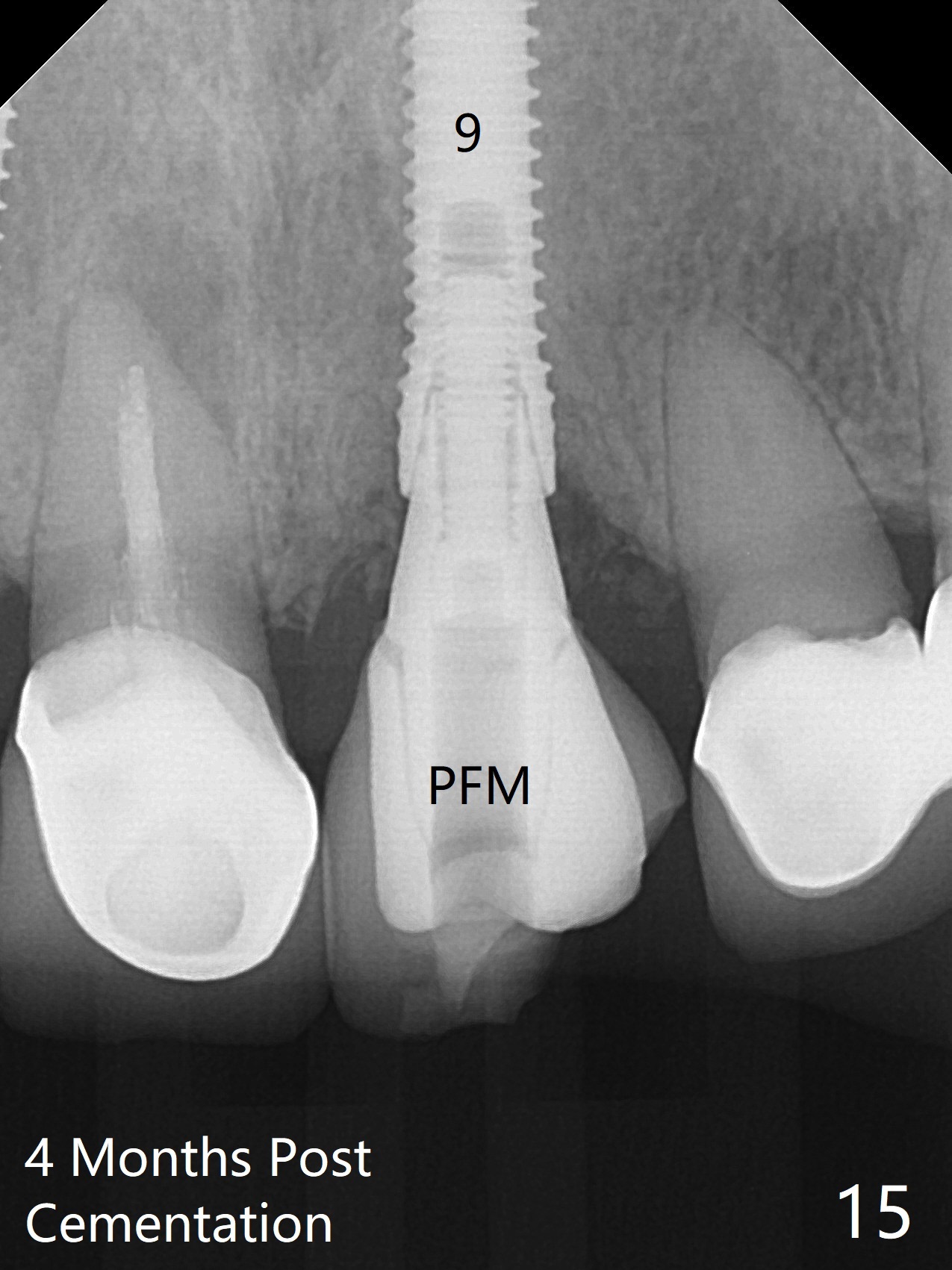
The buccal contour at #9 seems to be slightly concave preop (Fig.1,2 (*)). In fact the buccal plate is found to be lost when the tooth is extracted. Osteotomy is initiated as palatal as possible apical, but the occlusion dictates the coronal end of the osteotomy should be buccal, leaving the buccal gap ~ 2 mm for bone graft. The initial osteotomy (18 mm deep) appears to be close to the Incisive Foramen (Fig.3 blue dashed line). The nasal floor appears to be intact when the drill is removed. Subsequent osteotomy is adjusted so that the apical end of the osteotomy moves distal; when a 3.8x15 mm dummy implant is partially placed, there is clearance (Fig.4). It remains so when a definitive implant is seated (Fig.5); Vanilla graft is placed (Fig.5 *) before placement of a 4.5x5.5(3) mm abutment. More allograft is placed when an immediate provisional is fabricated (Fig.6 arrow and *). The gingiva remains to be recessive 1 month postop (Fig.7). It seems to be related to the bulky gingival margin of the provisional (Fig.8 *). After trimming the latter (Fig.9 *), the gingival margin immediately returns close to normal (Fig.10). The gingival margin is even between #8 and 9 two months postop, but the bone graft is exposed apically (Fig.11 ^). It may heals by itself. Otherwise debridement, regraft, PRF and suture are pending. The coronal portion of the socket heals 4 months postop (Fig.12). The gingival cuff forms by the immediate provisional (which is removed for impression) 4 months postop (Fig.13 *). While the full Zirconia crown at #7 remains intact (Fig.14), the PFM at #9 has porcelain chip (Fig.15). It is partially due to the occlusion; while the crown at #7 has clearance with the opposing dentition (Fig.16 *), the one at #9 has no. The access hole at #9 (Fig.17 *) seems to weaken the crown structure. There is no access hole at #7. No solid posterior support is another contributing factor for chip (Fig.18). The buccal plate has mild atrophy at #7 and 9 (Fig.19 *). A piece of bone graft is being expelled apically at #9 (Fig.20 >) and is removed subsequently (Fig.21). Before impression for repacking porcelain, the opposing incisal edge has been shortened (Fig.22 arrows, as compared to Fig.16). Since the ideal access hole is at the incisal edge (Fig.25 black circle), buccal to the existing one (Fig.24 A), the abutment is torqued before the repaired crown is recemented (Fig.23). Finally the crown has occlusal clearance (Fig.26). Porcelain chips again around the access hole of PFM 1.5 years post 2nd cementation. The dense bone at the crest (*) cannot explain why the abutment is not loose, since it remains incompletely seated (>). As it was trimmed short, an angled abutment is used (Fig.28). The coronal end is lingual, while #9/24 is edge to edge. The lingual aspect of the coronal end of the abutment is heavily trimmed to reduce bulkiness. To prevent chip, Zirconium crown will be fabricated in spite of the fact that it does not match the PFM of #8 (potential shade discrepancy). The patient is pleased with the new Zirconia crown (Fig.29).
Return to
Upper
Incisor Immediate Implant,
Armaments,
#7
Xin Wei, DDS, PhD, MS 1st edition 06/14/2018, last revision 10/20/2020