



|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Two Stage
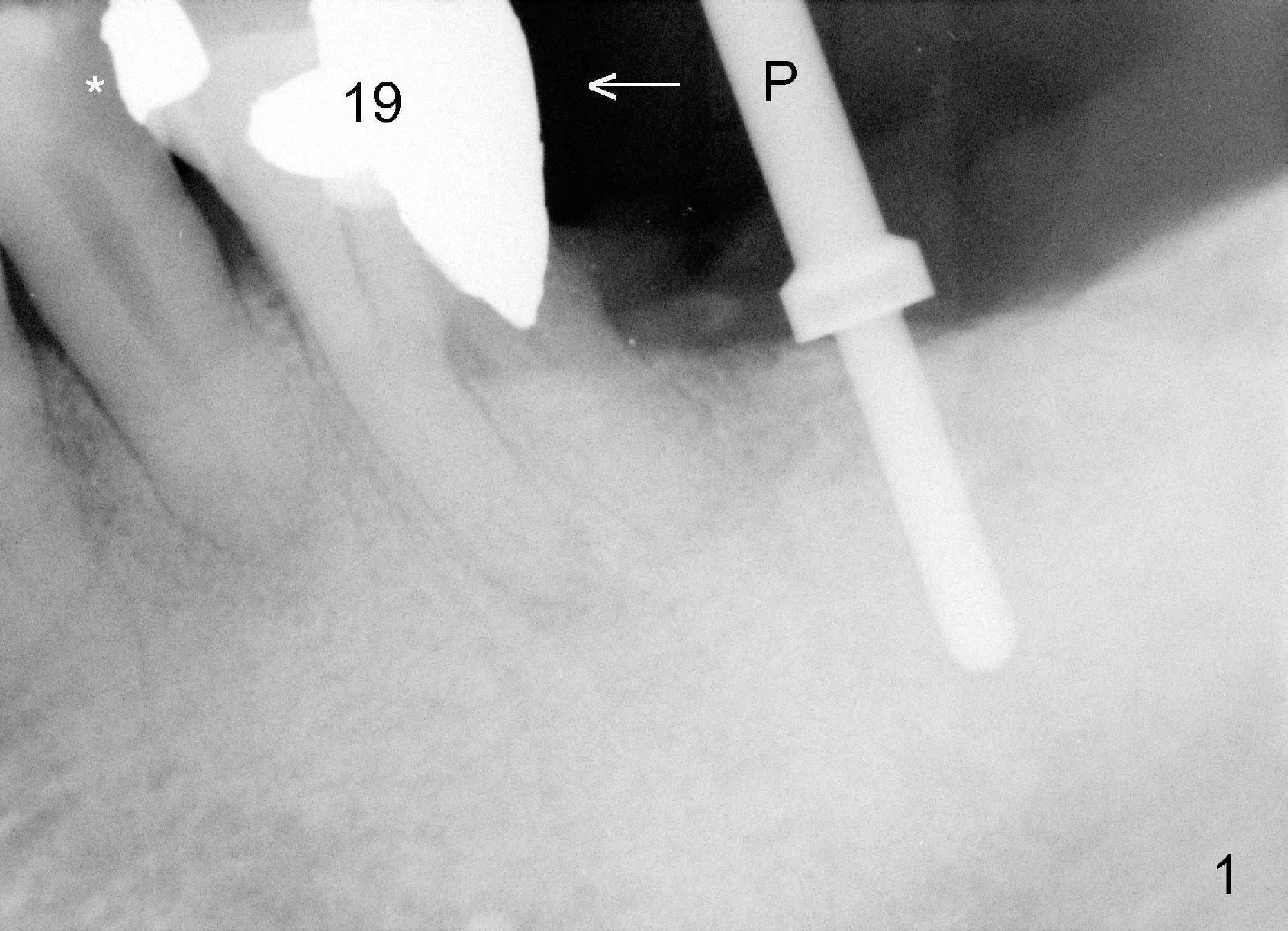
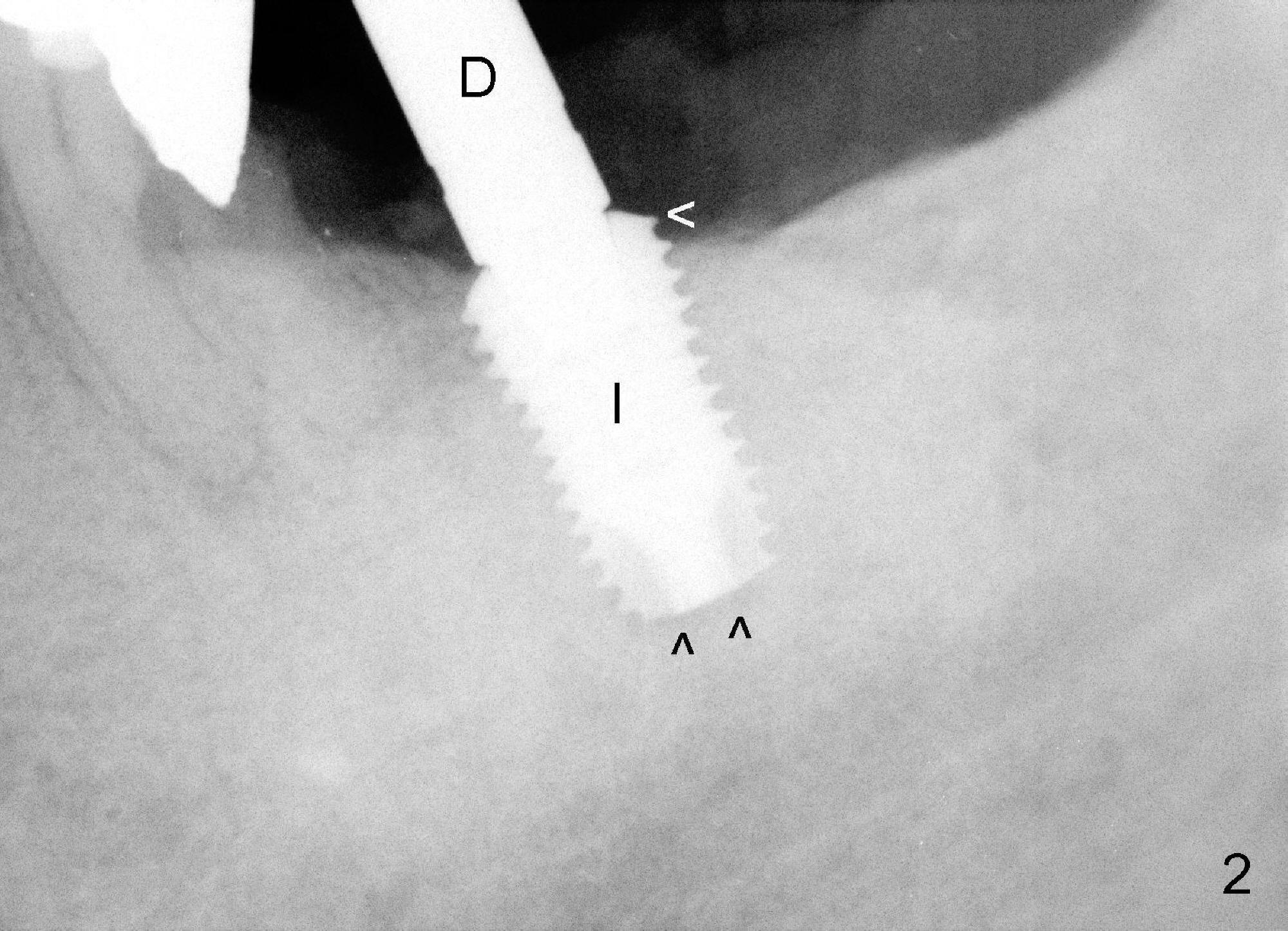
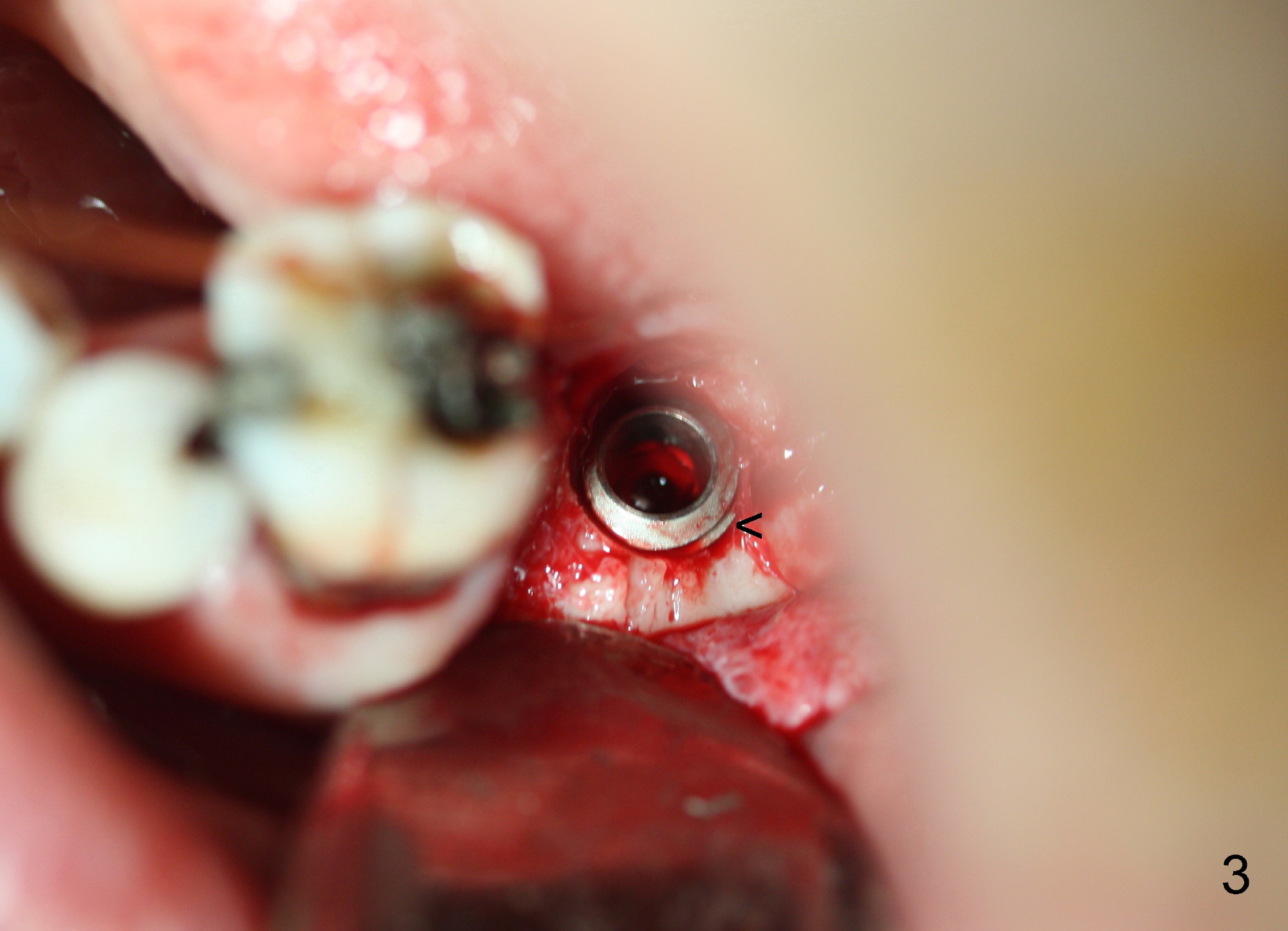
The 69-year-old male is a dental phobic with poor dentition. He wants to an implant at the site of #18 first and refuses to have the tooth #11 (with asymptomatic apical abscess) extracted. To reduce chance of post-implant infection, the implant is placed in a two stage manner. The distal amalgam overhang of the tooth #19 is removed by Piezo scaler (Fig.1). An incision is made. After a 2 mm pilot drill, a parallel pin is inserted; it appears that the coronal end of the trajectory should be leaned mesially (Fig.1 arrow). Since the ridge is wide, an extra wide implant is placed (Fig.2 I: 5.9x10 mm with insertion torque >50 Ncm) with one distal thread exposed (Fig.2,3 <). The disto-occlusal caries of the tooth #20 (Fig.1,4 *) is going to be excavated.
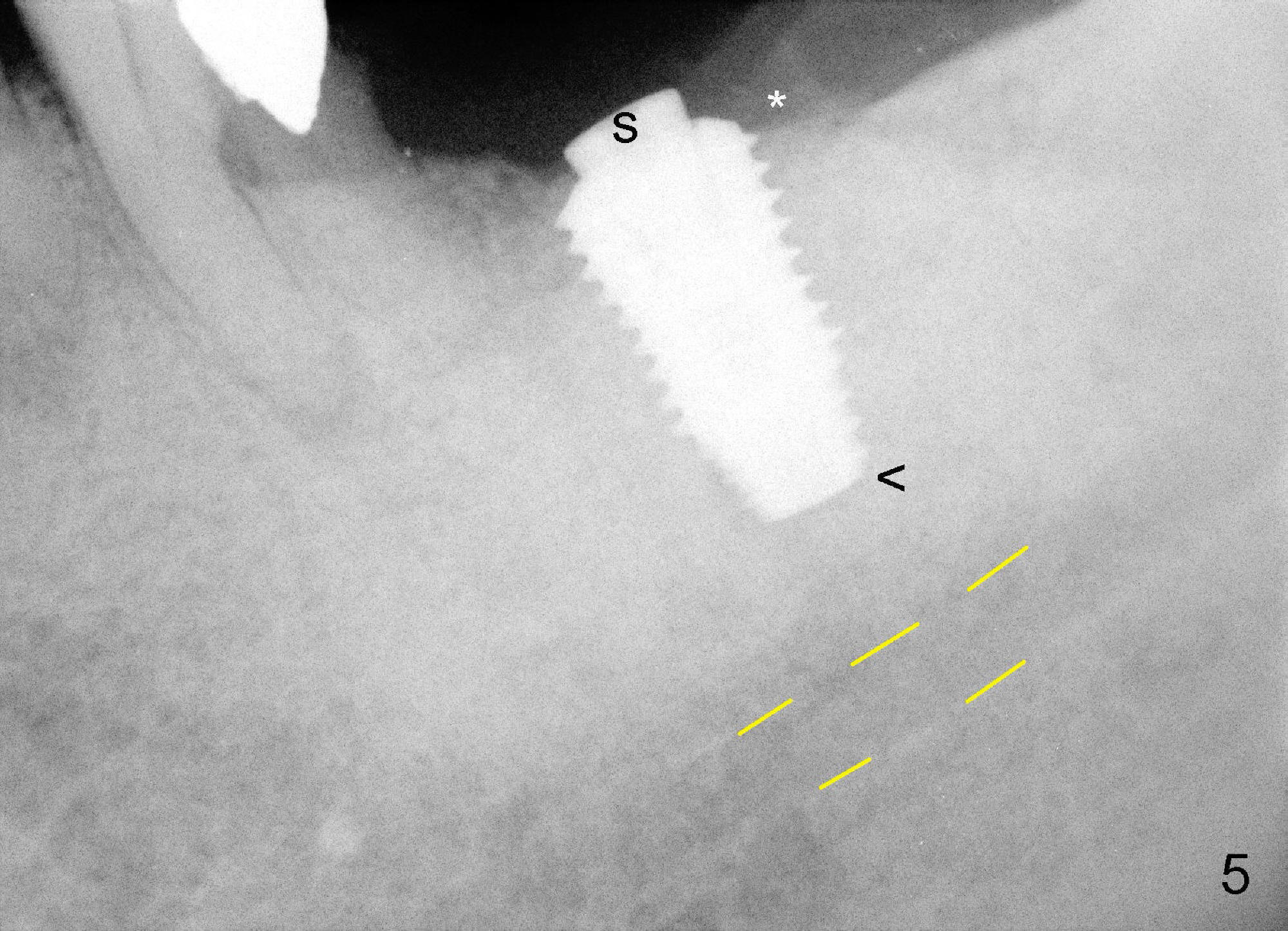
The implant is torqued down further (Fig.5 <, as compared to double ^ in Fig.2). The remaining distal exposed thread is covered by autogenous bone harvested during osteotomy (*). The graft is then covered by collagen dressing, which is held in place by a partially placed healing screw (S). The wound is closed by 4-0 Chromic gut suture and perio glue. The patient is instructed to continue oral Amoxicillin and Chlorhexidine mouth rinse postop.
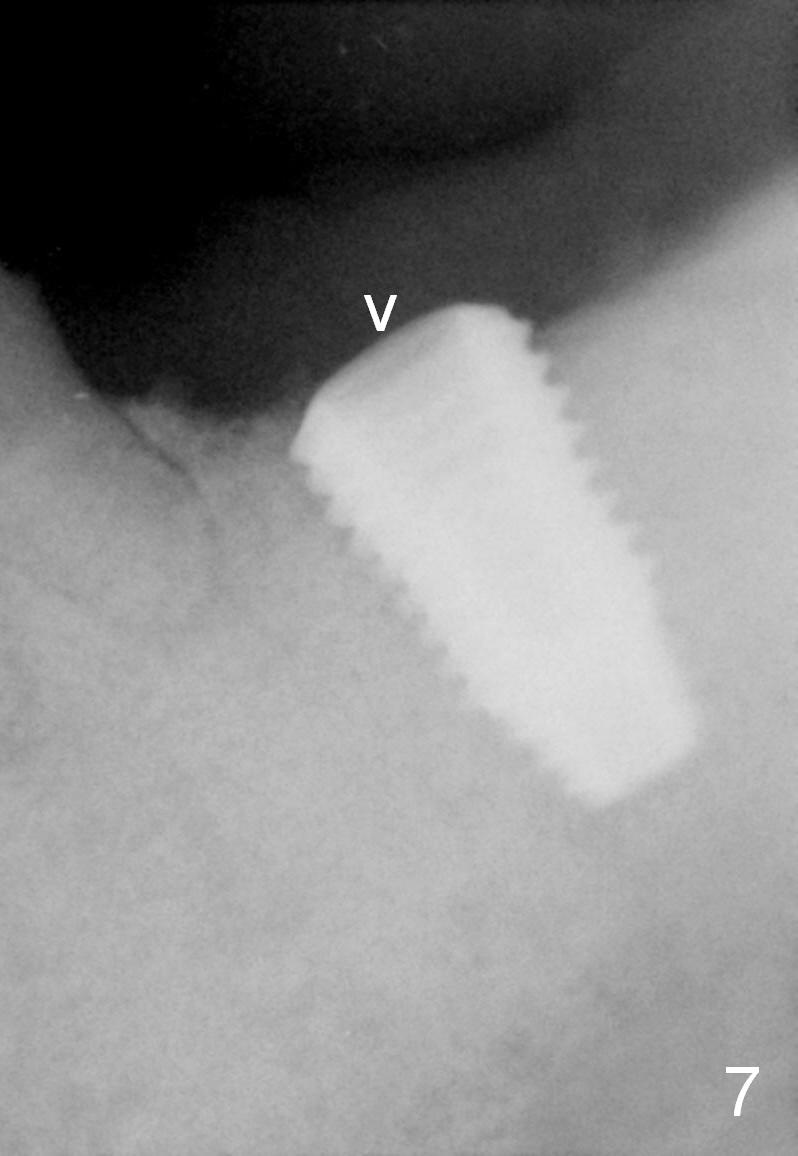
The patient returns 8 days postop, asymptomatic, but the wound is erythematous. Amoxicillin is refilled for extra one week. Two months postop, the incision heals (Fig.6); the healing screw is lost (Fig.7 arrowhead), while bone graft retains (Fig.8 *).
Eight months post cementation, the patient is pleased to let us know that he can chew peanuts with the implant crown (Fig.9) and asks for a 2nd implant.
Return to Professionals
Lower Molar Immediate Implant #6
27
Xin Wei, DDS, PhD, MS 1st edition 01/09/2015, last revision 09/22/2018