


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
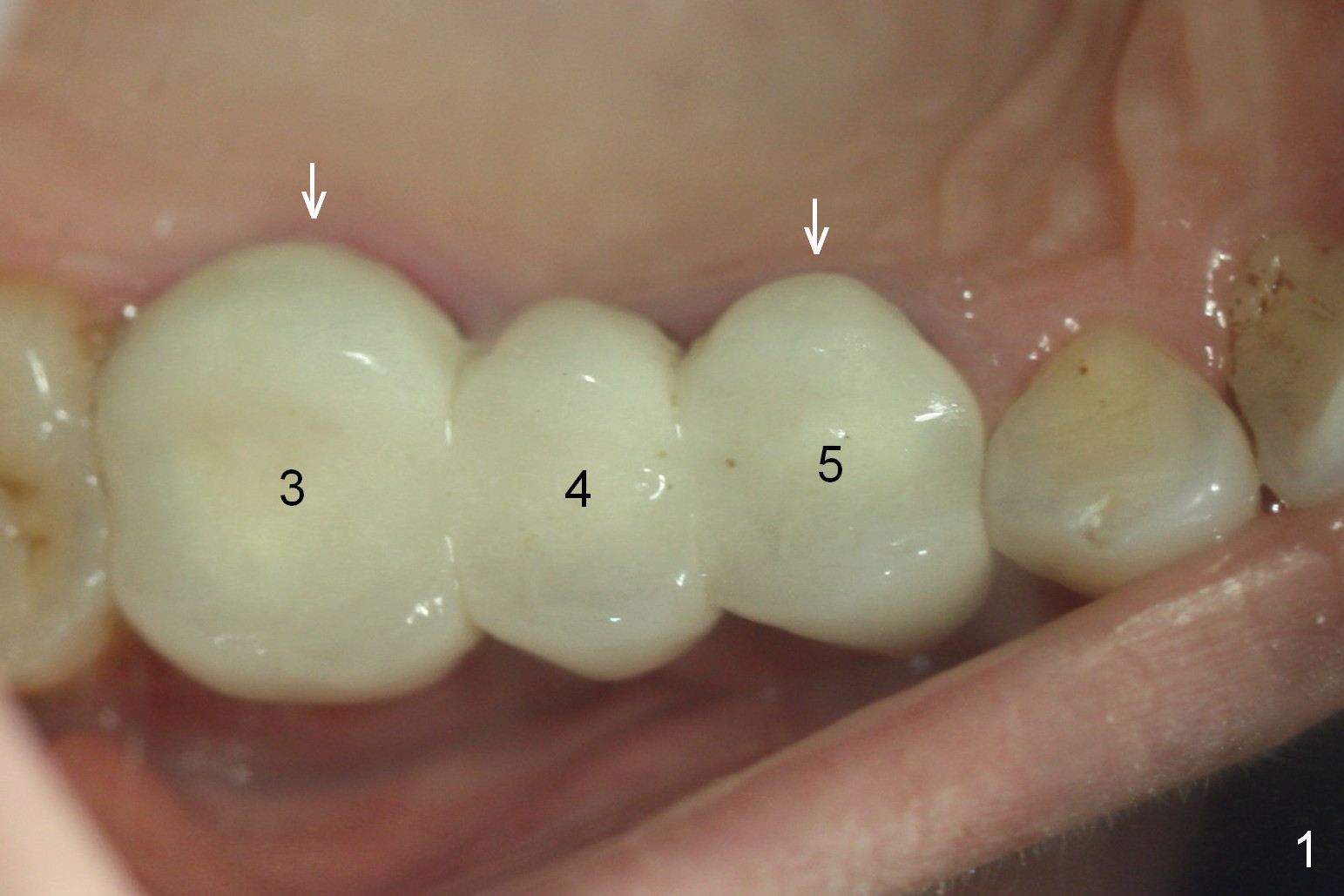
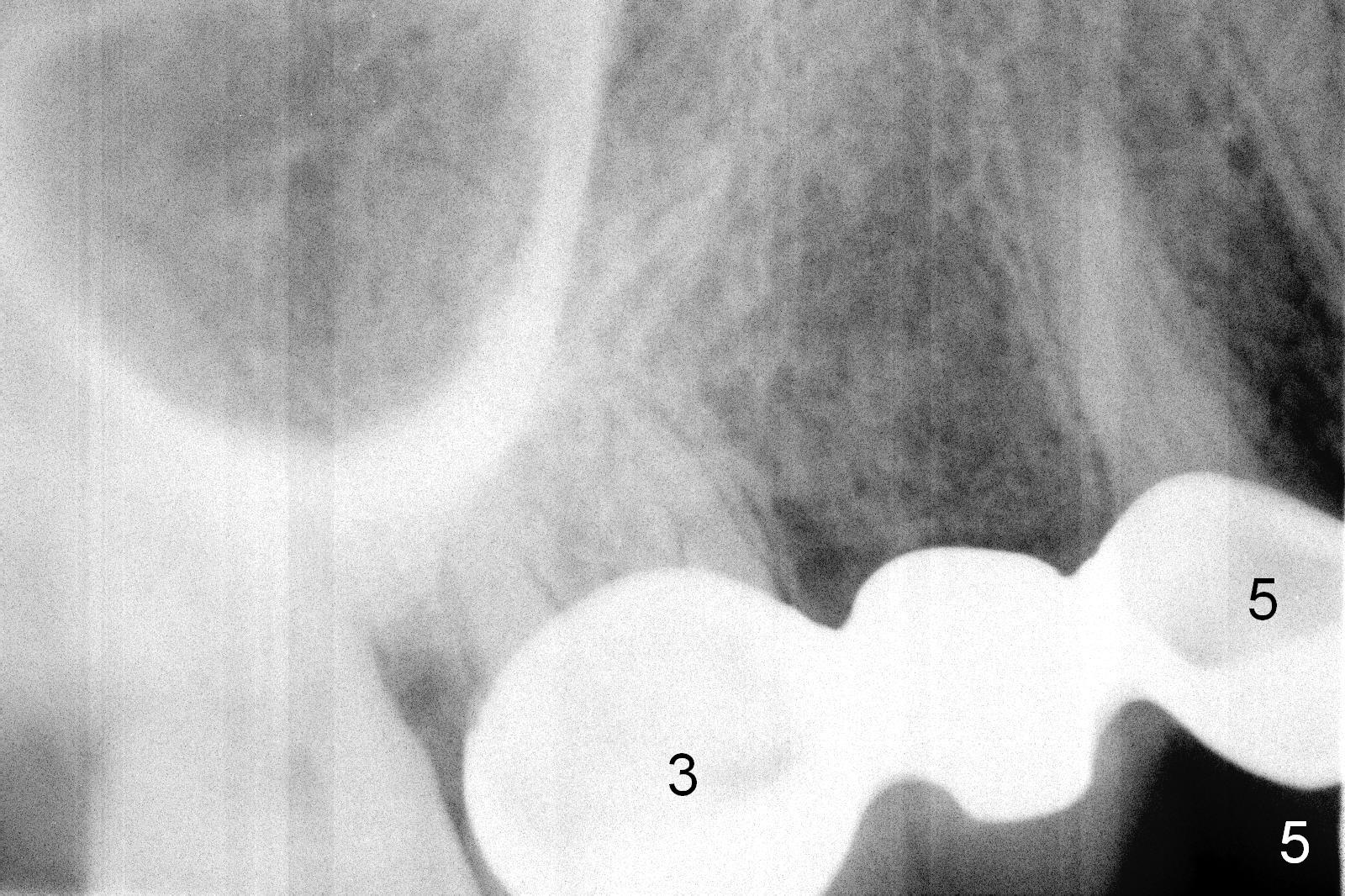
Over-Contoured Bridge and Gingival Hemorrhage
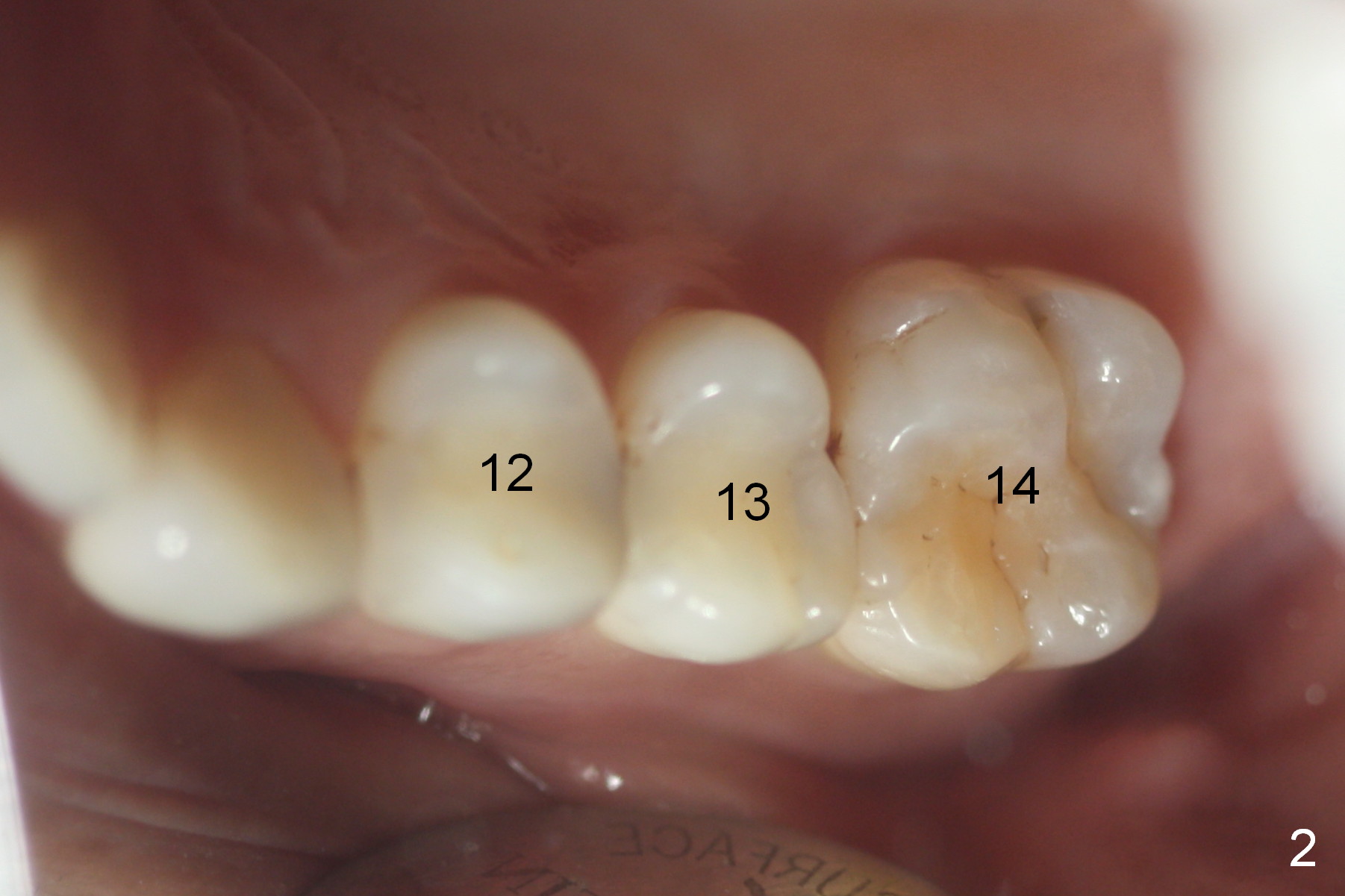
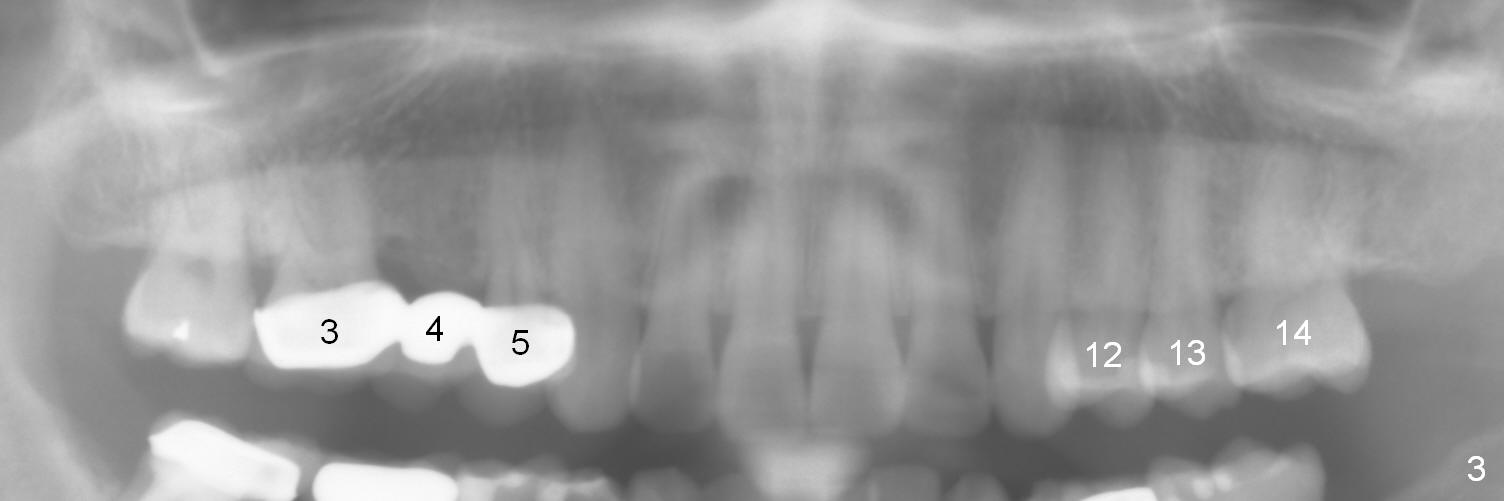
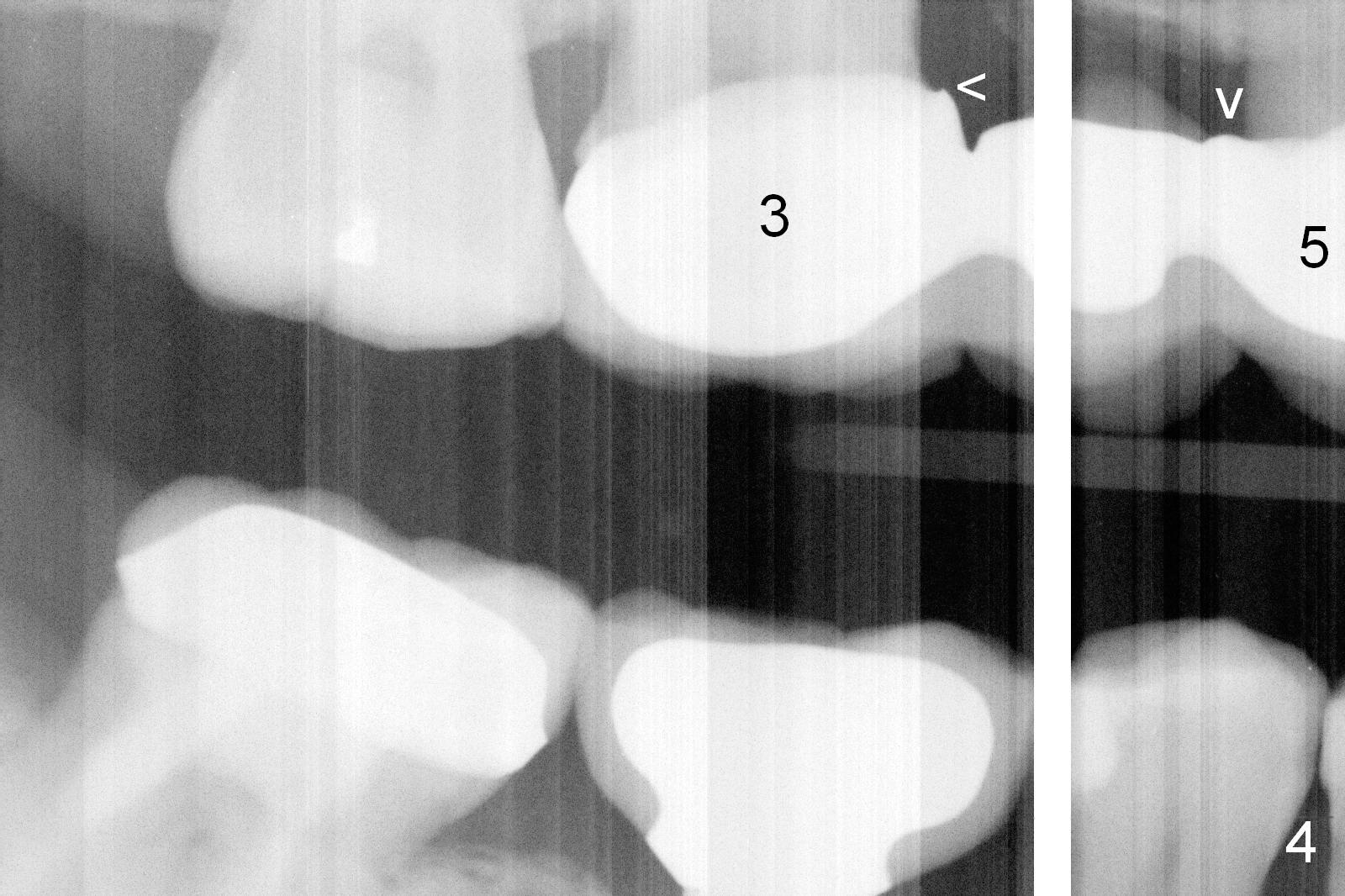
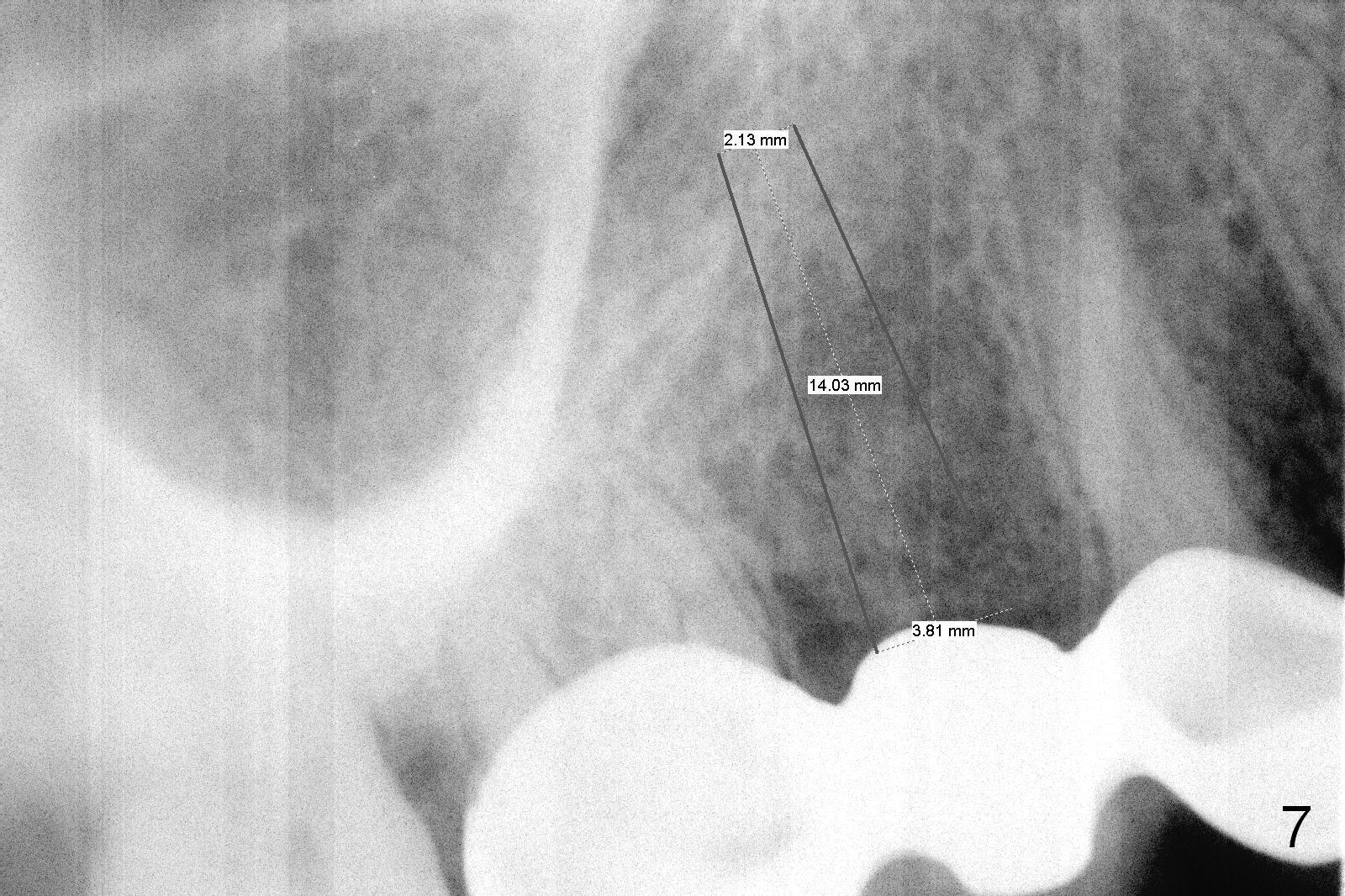
Ms. Li, a 34-year-old lady, had the upper right fixed partial denture made by an unlicensed dentist in California 10 years ago (Fig.1: #3-5). The gingival margin palatal to the retainers is erythematous (Fig.1 arrows). The patient's chief complaint is gum bleeding. The retainer at #3 is over-contoured buccopalatally (Fig.1, as compared to #14 in Fig.2), while the one at #5 is over-contoured buccopalatally and mesiodistally (compare to #12 in Fig.2). Panoramic X-ray (Fig.3), bitewing (Fig.4) and periapical film (Fig.5) all confirm that the bridge is over-contoured and that the retainers #3 and 5 have open margin (Fig.4 arrowheads). To improve oral hygiene and save the abutment teeth #3 and 5, it is in the patient's best interest to remove the bridge, place an implant at #4 and fabricate single-unit crowns at #3 and 5. Three to four months later, pyogenic granuloma develops between #4 and 5 (Fig.6 *) with generalized gingival erythema apically. The pontic at #4 and the retainer at #5 are to be removed first. An implant will be placed at #4 (Fig.7) with conjoined provisional at #4 and 5. The initial depth of osteotomy is 13 mm with Sinus Master Kit.
Eleven days later when the patient returns for bridge sectioning and implant placement, the pontic infection extends distally (Fig.8 <). When the bridge is sectioned, the pontic mucosa appears unsuitable for implant surgery (Fig.9). The patient is discharged after fabrication of a provisional at #5. She is rescheduled for implant placement 17 days later. IBS implant is to be placed because of its dual system. If the bone is soft, go to the bone expansion route. Otherwise, choose the traditional method: drilling.
Return to Upper Premolar Immediate Implant,
Posterior Immediate Provisional,
IBS
Xin Wei, DDS, PhD, MS 1st edition 03/15/2016, last revision 01/19/2018