
,%20mineralized%20graft.jpg)
,%20graft.jpg)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|||
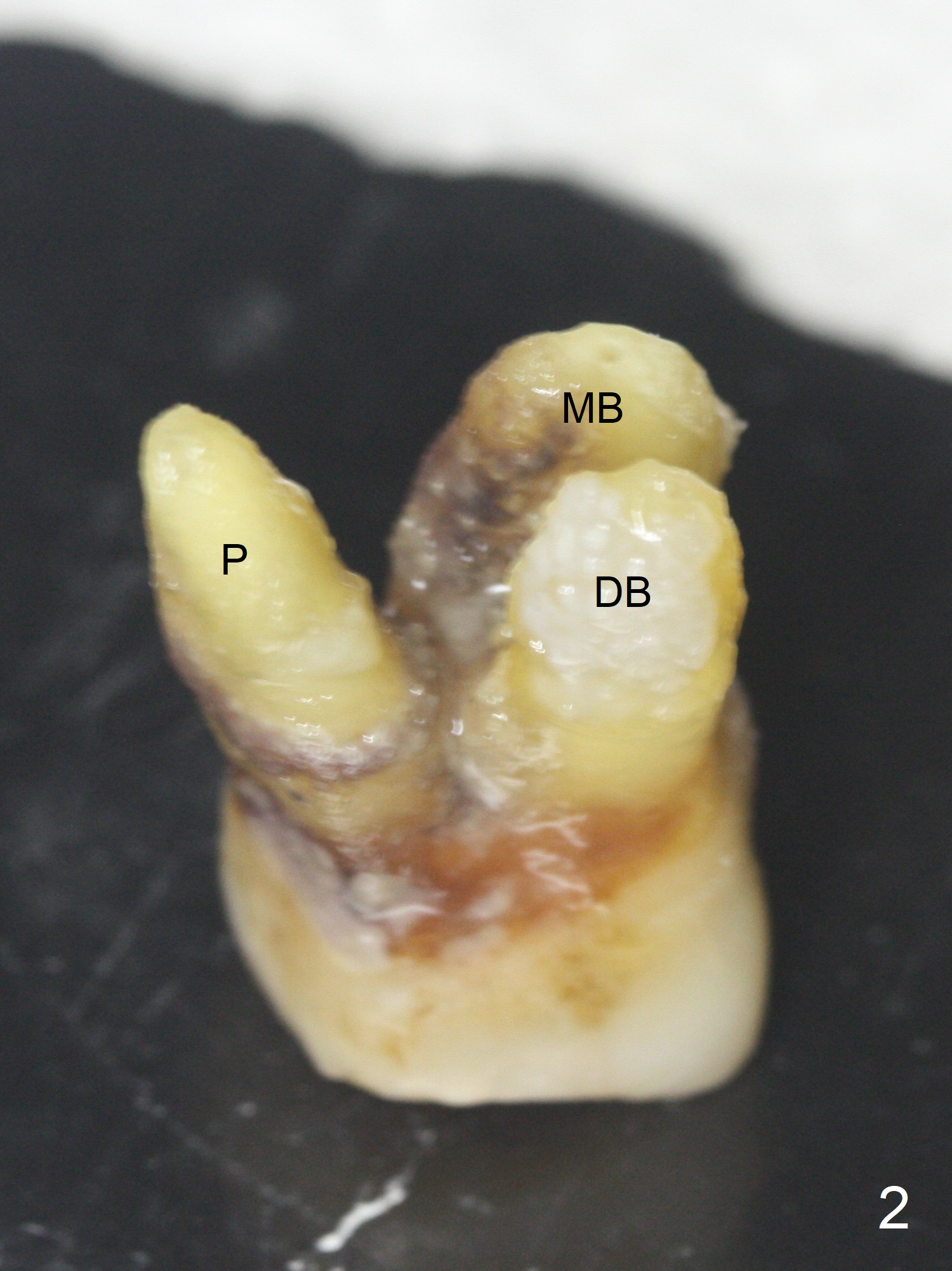
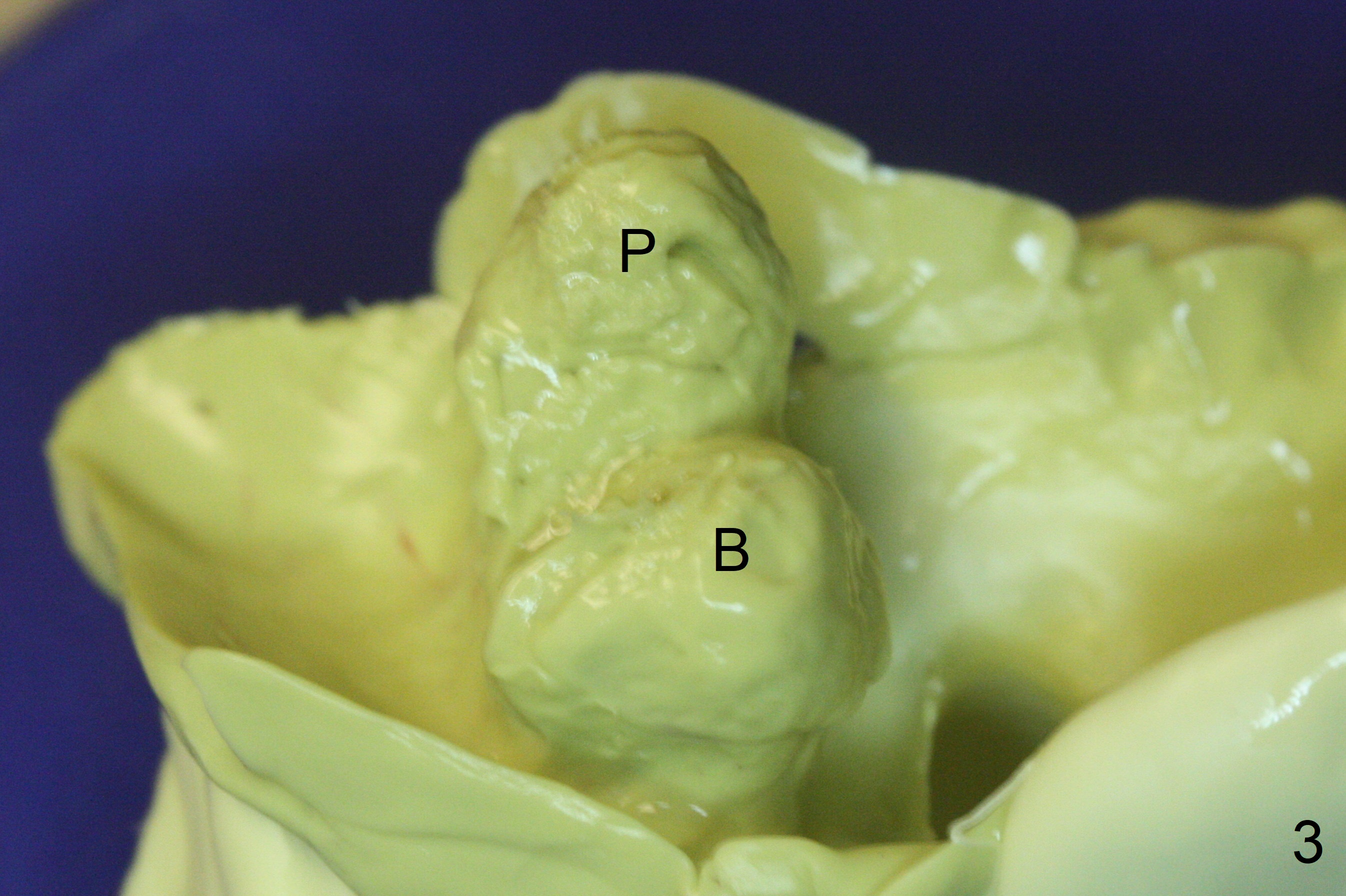
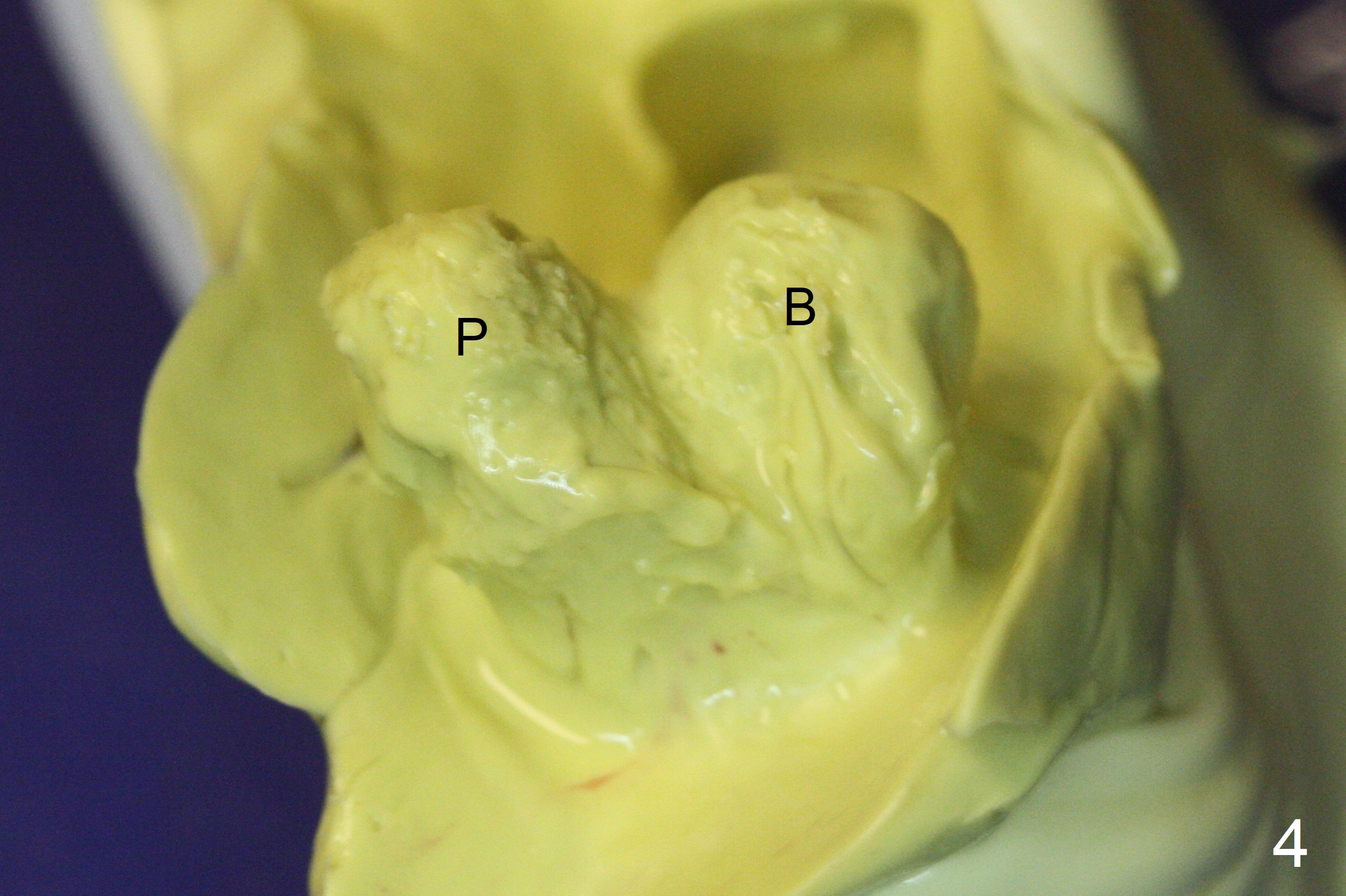
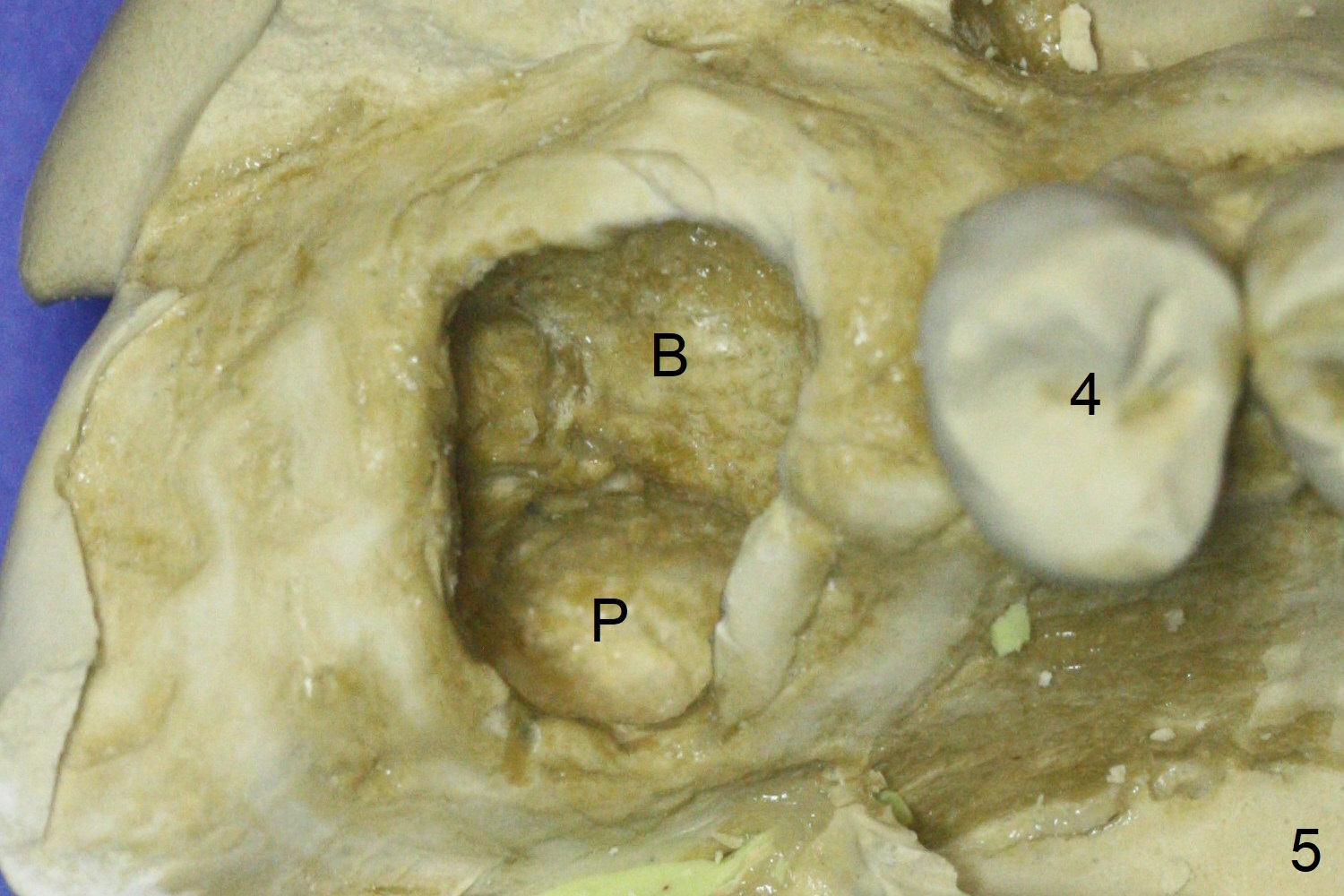
Buccal Socket Placement
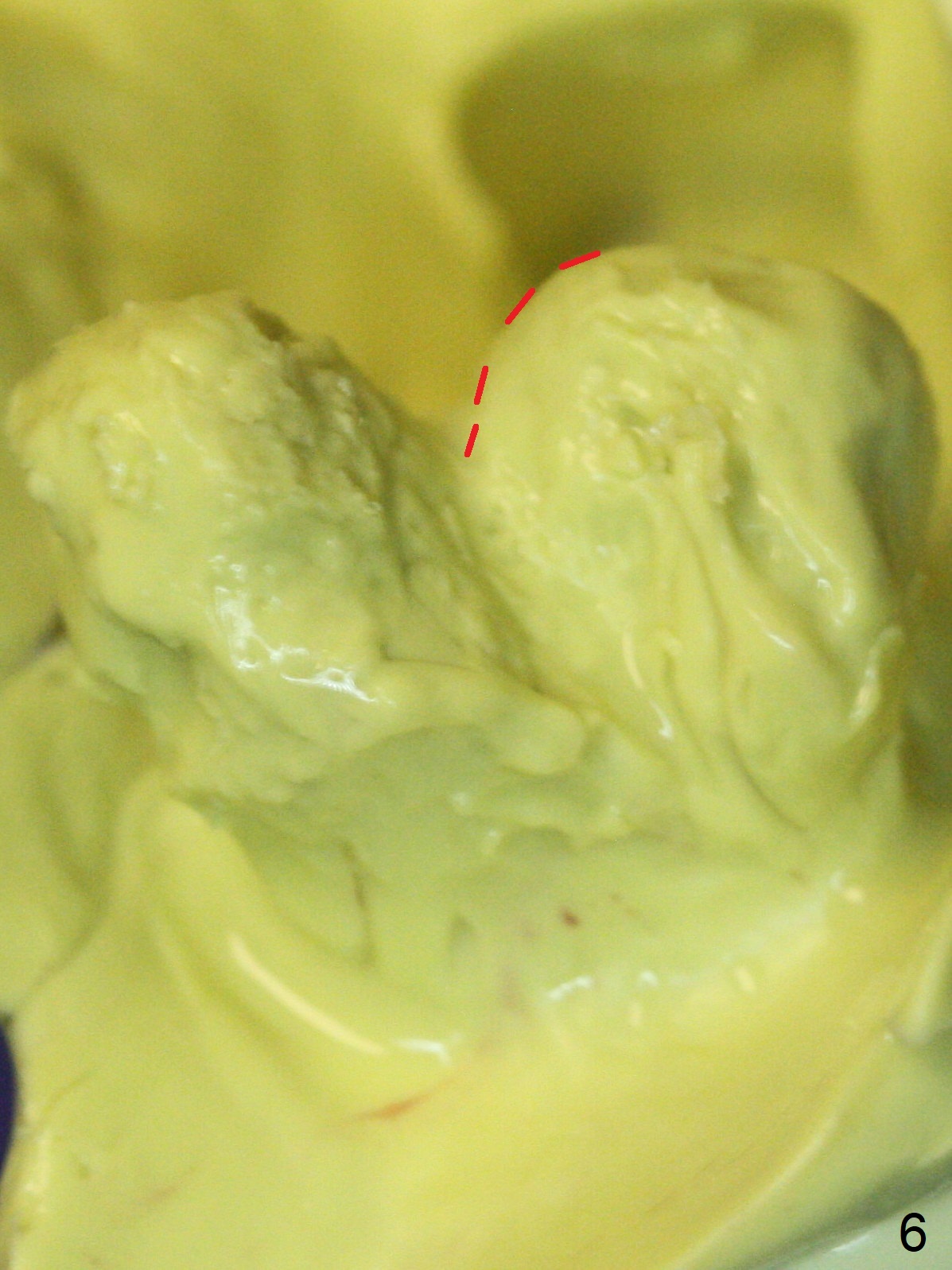
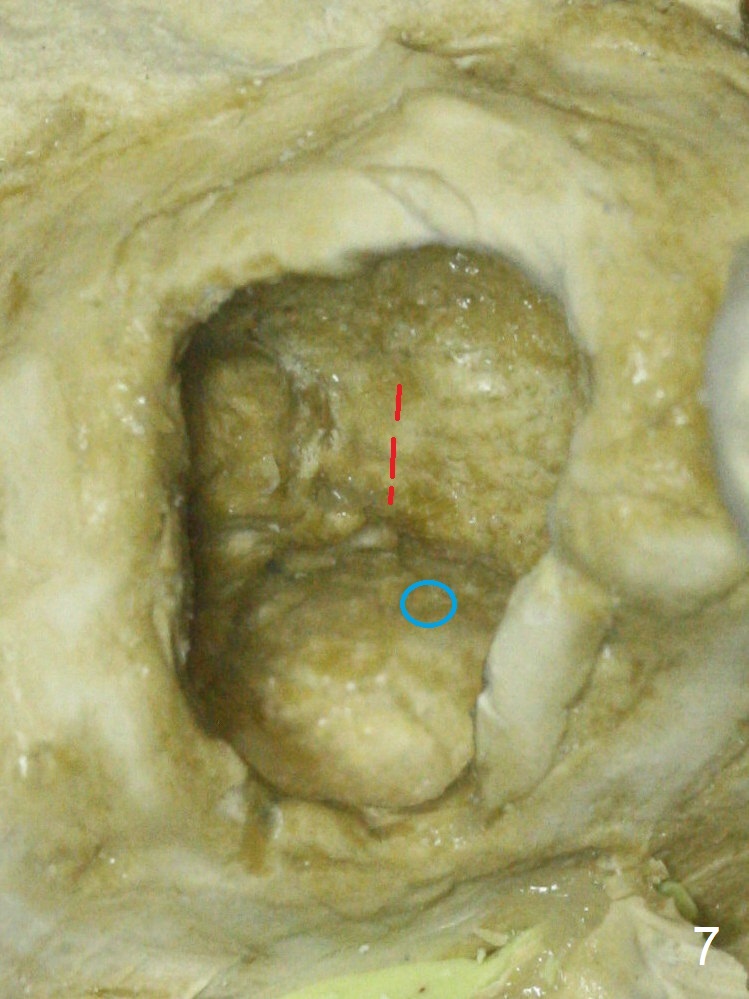
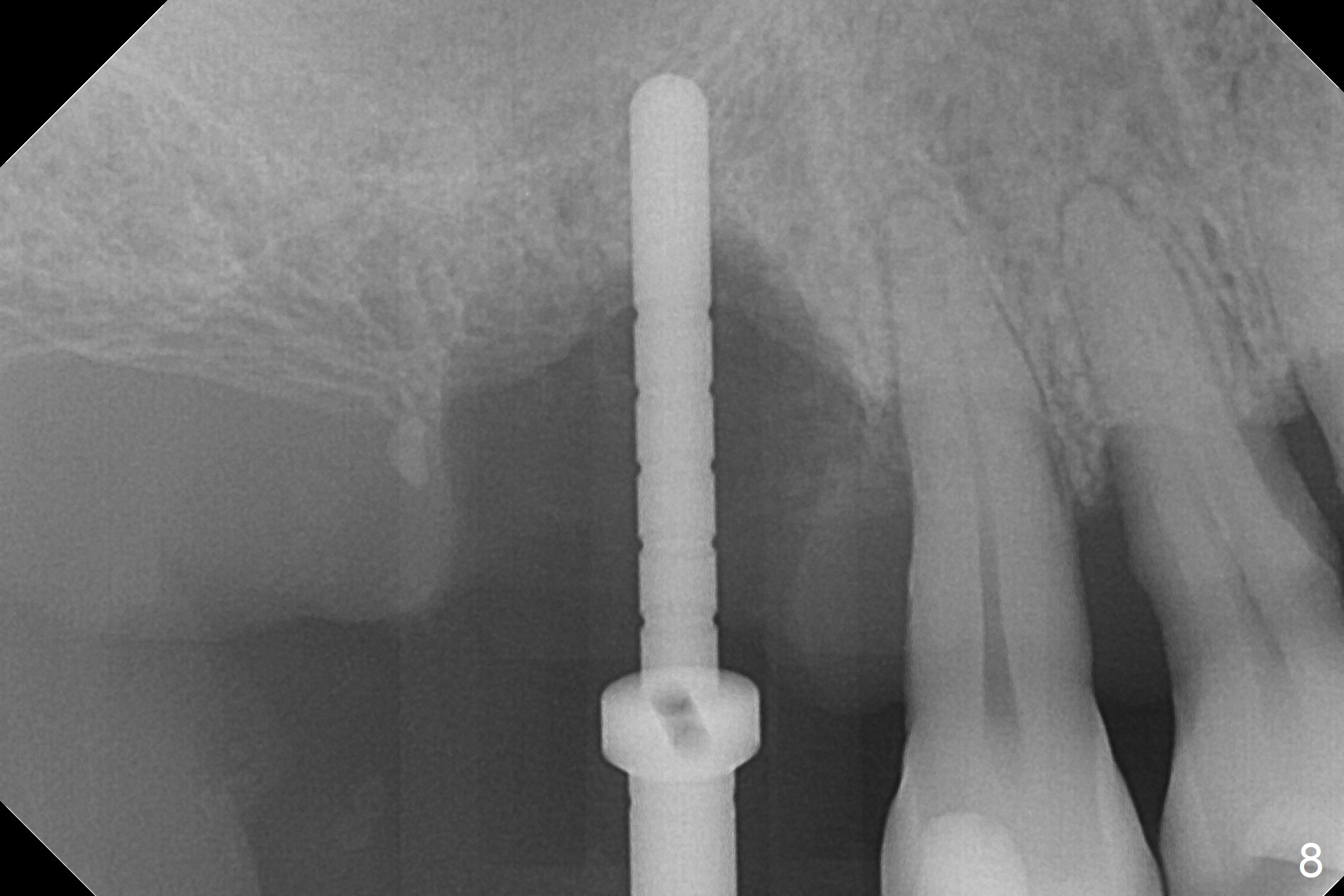
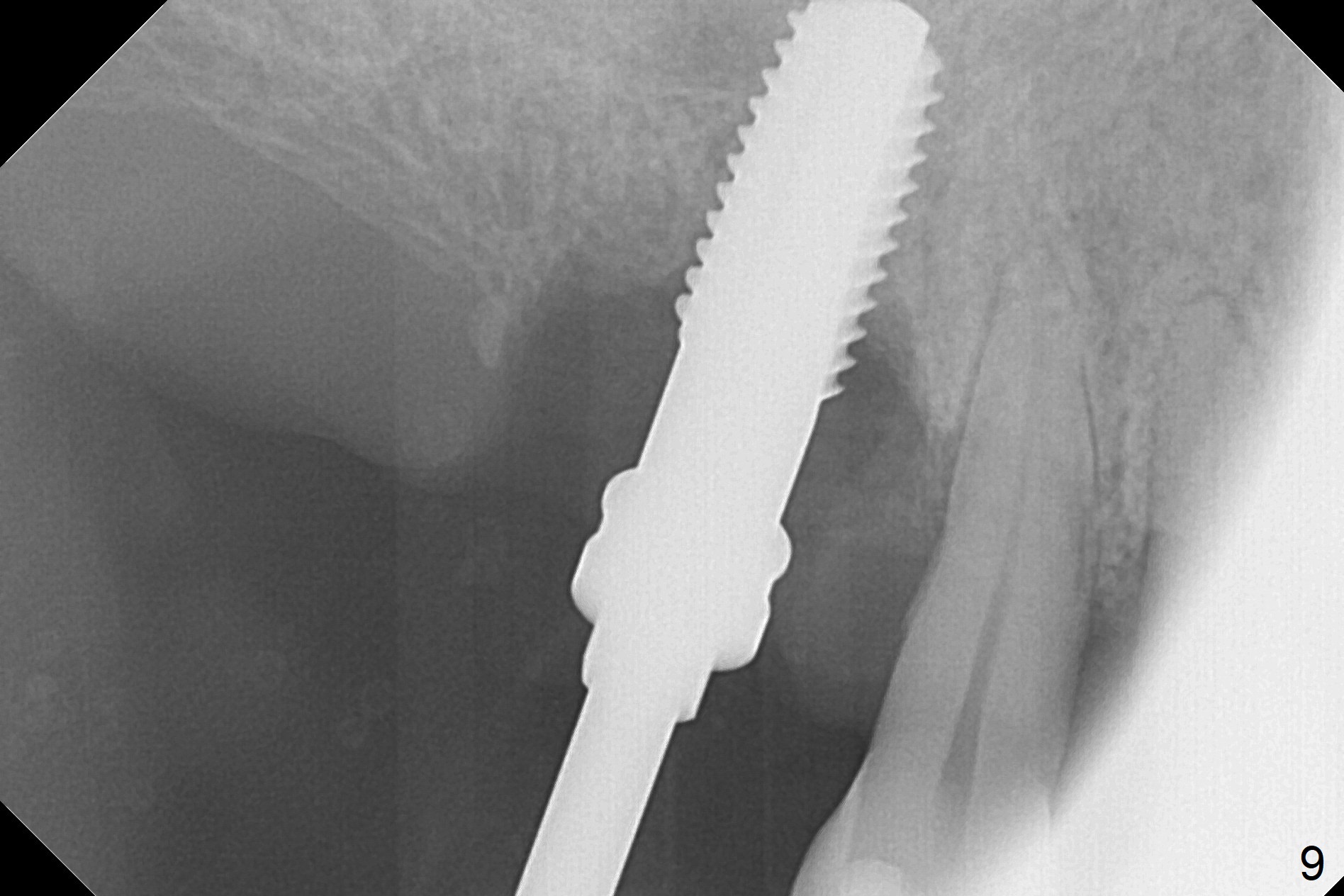
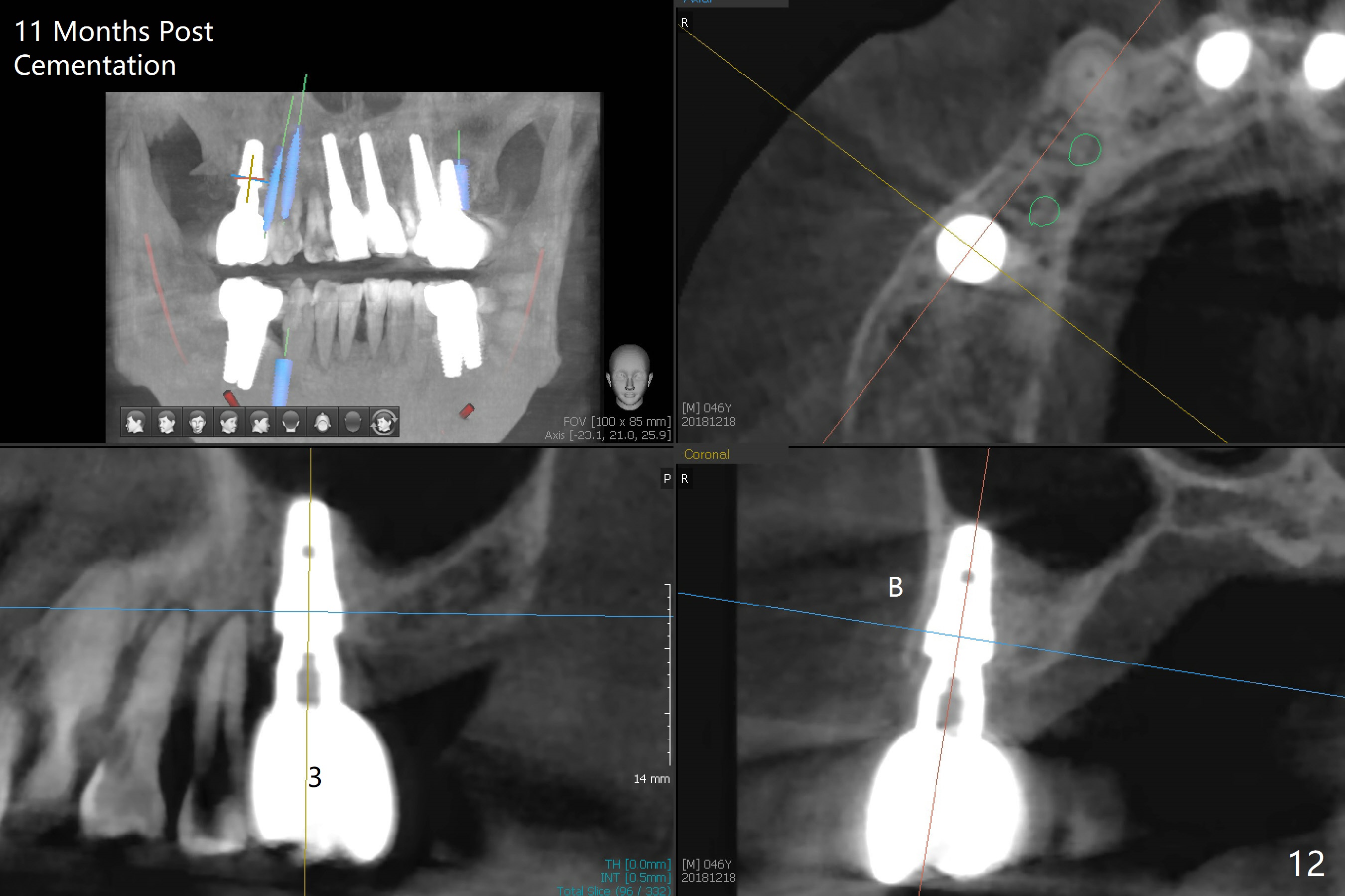
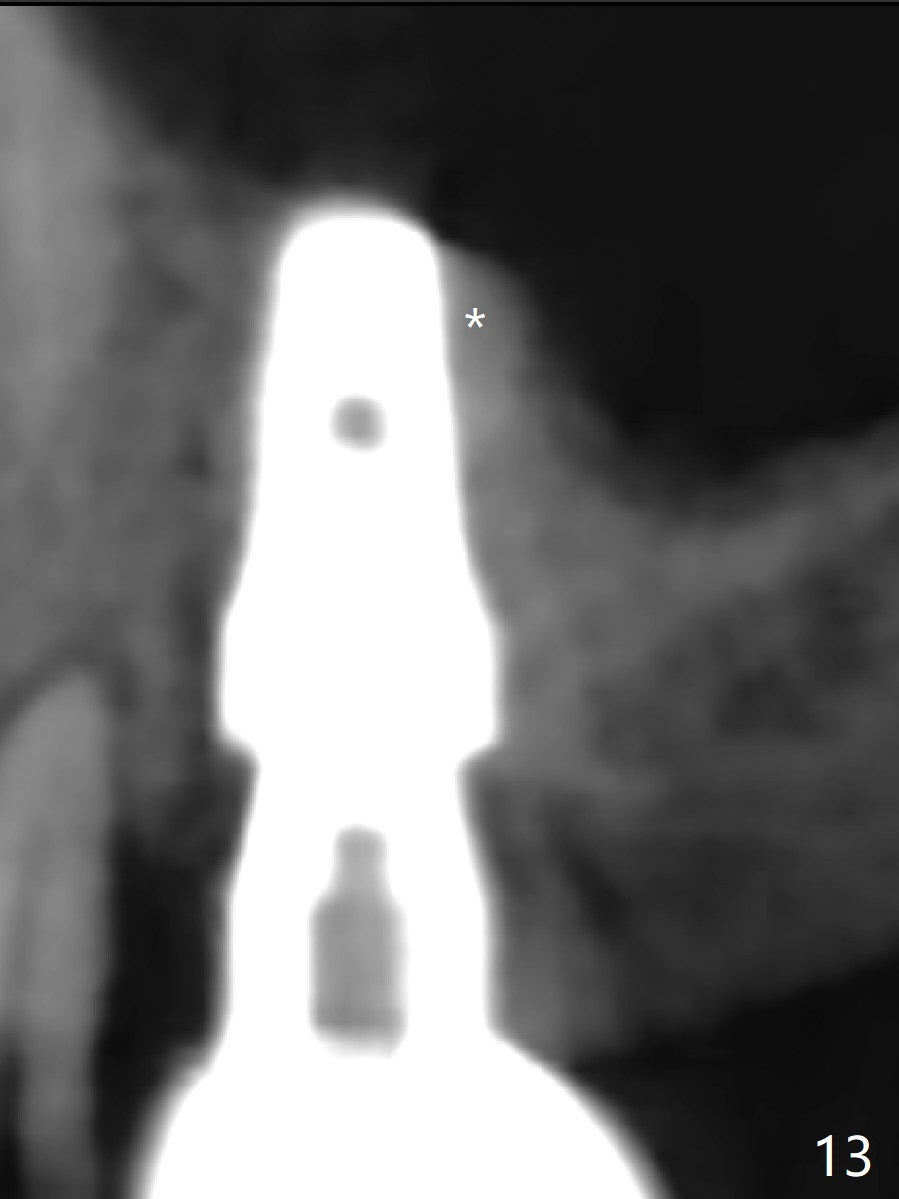
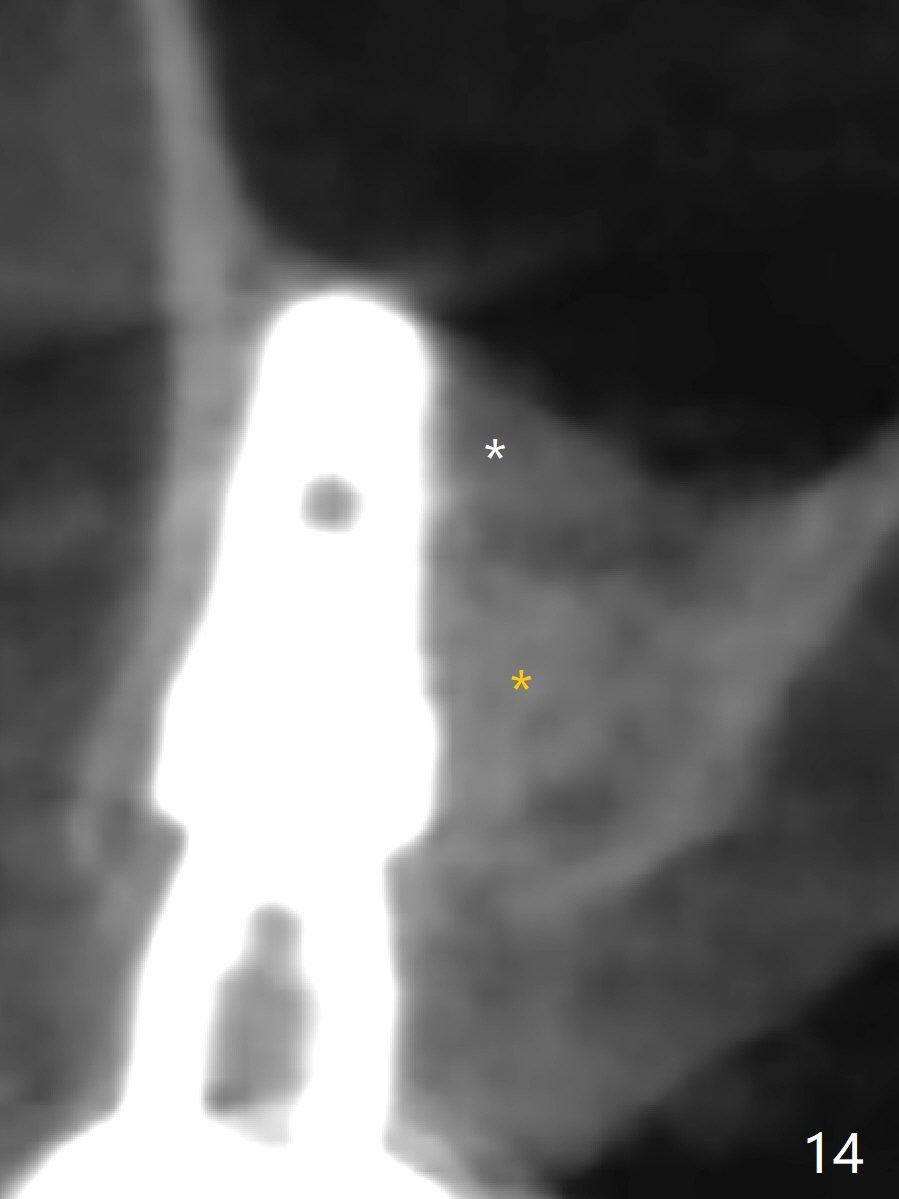
After extraction of the tooth #3 (Fig.1,2), the palatal socket (P) is as wide as the buccal one (B; Fig.3,4 (socket impression)), as compared to the roots), suggesting bone loss is more severe palatally than buccally. There is a circular area in the buccal slope of the palatal socket, in which the bone looks thin (purplish: presumably the sinus membrane underneath, Fig.5,7 (blue circle)). It appears that the palatal slope of the buccal socket (Fig.6, 7 red dashed line) is the most appropriate site for osteotomy (Fig.8). Prior to inserting 5.3 mm tap drill (Fig.9), the mesiopalatal region of the osteotomy (corresponding to the blue circle in Fig.7) perforates without sinus membrane tear. A small piece of Osteogen plug is placed in the perforation before inserting a 5.3x10 mm SM implant (Fig.10,11). Following placement of another piece of Osteogen plug in the palatal socket and of a 4.8x7(6) mm abutment, mineralized cortical and cancellous bone is placed (*). Collagen plug and an immediate provisional are used to close the socket opening. CT taken 11 months post cementation shows that the implant is placed within bony boundary, although buccally (Fig.12 B). Bone graft seems to heal in the sinus (Fig.13 (sagittal section),14 (coronal section) white * (Osteogen plug) and in the socket (brown * (allograft and Osteogen)).
Return to
Upper
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS,#28,
31,
14,
4/5
中文
Osteogen Plug for Socket Preservation
Xin Wei, DDS, PhD, MS 1st edition 07/10/2017, last revision 01/05/2019