


,%203.8x15.jpg)
,%20then%20redirect.jpg)












%20m%20postop.jpg)




|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
It is not Too Late to Change Trajectory
The dentition is poor except #6 and 8 (Fig.1). The gingiva is erythematous at #9-11 (Fig.2). The teeth #9 and 10 are extracted first; a 4x16 mm UF implant is placed at #9, while a 2 mm pilot drill is at the site of #10 (Fig.3). The implant at #9 is placed deeper with placement of 4.5x5.5(5) mm abutment; a 3.8x15 mm implant is placed at #10 initially (Fig.4). While the latter is placed deeper, a 4x16 mm implant is placed at #11 (Fig.5 after removal of #11-15 FPD (fixed partial denture)). In fact the trajectory at #11 is not difficult to be changed with 2 mm drill (Fig.6). After use of 3 mm drill, the implant is reinserted at #11 with ideal trajectory (Fig.7). After further seating of the implant at #11, graft is placed in the remaining sockets of #9-11 (Fig.8 *; later more graft is placed mesial to #11 implant (^)). Finally, a 4.5x7(5), 4.5x15° B (4) and 5.5x7(5) mm abutments are tightened and prepared (Fig.9) for splinted provisional at #9-10.
The second part of the upper left quadrant surgery involves implant placement at #15. What should be done next?
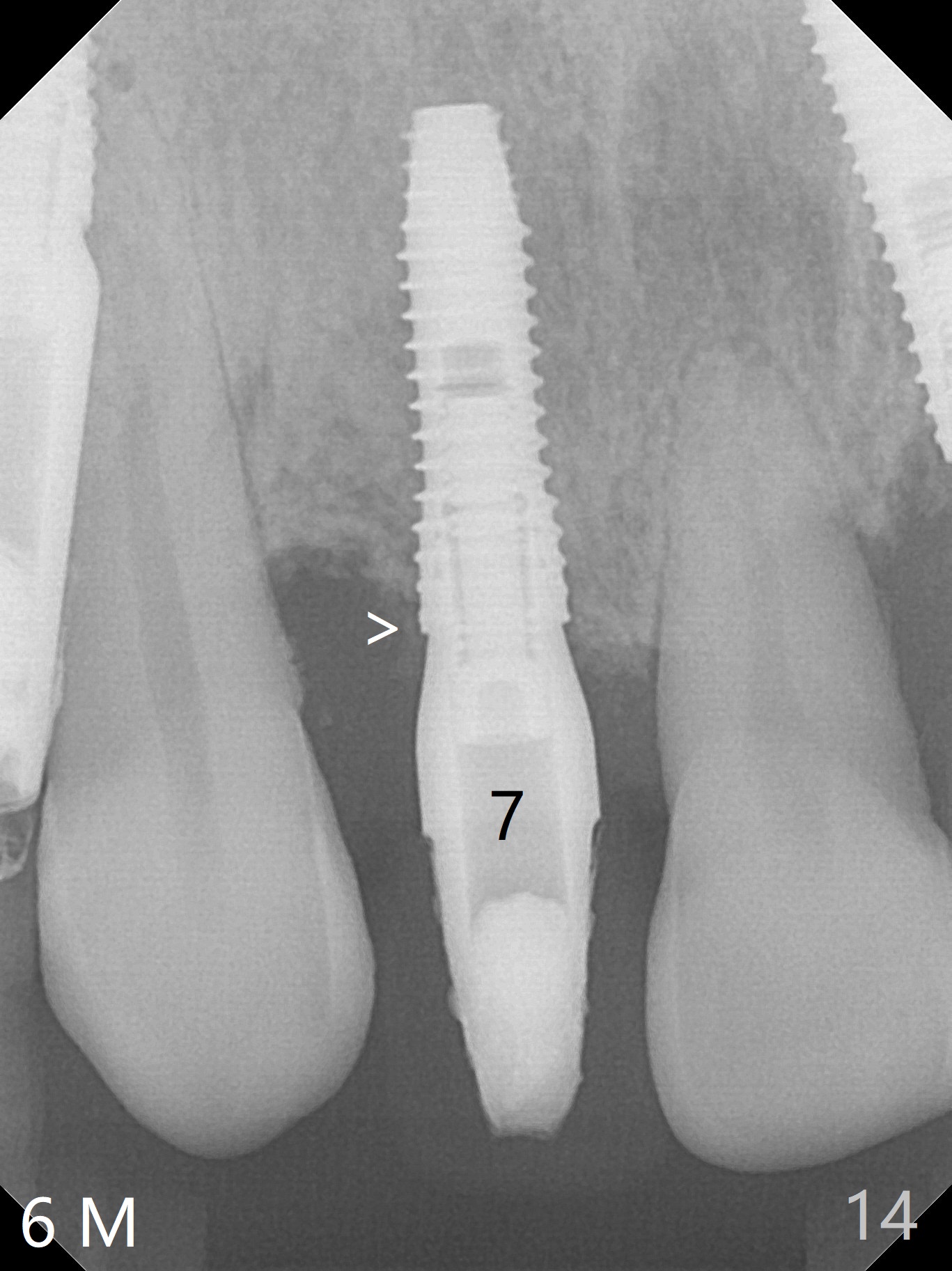
The patient returns 8 days postop, uncomfortable with overhang in the provisional (Fig.10 *). The sockets appear to be healing with loose bone graft (Fig.11) when the provisional is removed for trimming (Fig.12). Six (for #7,13) and seven (#9-11,15) months postop, the soft (Fig.13,17) and hard (Fig.14-16,18) tissues heal. It appears that the trajectory at #9,11 and 13 should be changed by using angled abutments (Fig.18,19 (panoramic X-ray taken 2 months earlier)) before provisional and final restoration.
In fact angled abutments are used at #11 and 13 (4.5x15 degree (5 mm)A) with a straight abutment at #15 (5.5x4(4) mm).
There is 1-2 thread exposure mesial and distal at #10 two years postop (Fig.20'), which may be related to the small fistula labially (Fig.20 >). It appears that the implant at #10 was placed too high (Fig.21) and labially (Fig.22). In fact the bridge fractures between #12 and 13 during pandemic.
Return to
Full Mouth Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table), IBS, #2,3,5,
7
Xin Wei, DDS, PhD, MS 1st edition 02/24/2017, last revision 08/26/2020