
,%20Vera.jpg)


|
|
|
|
|
|
|
|
|
|
|
|
|
||
Control Osteotomy Depth
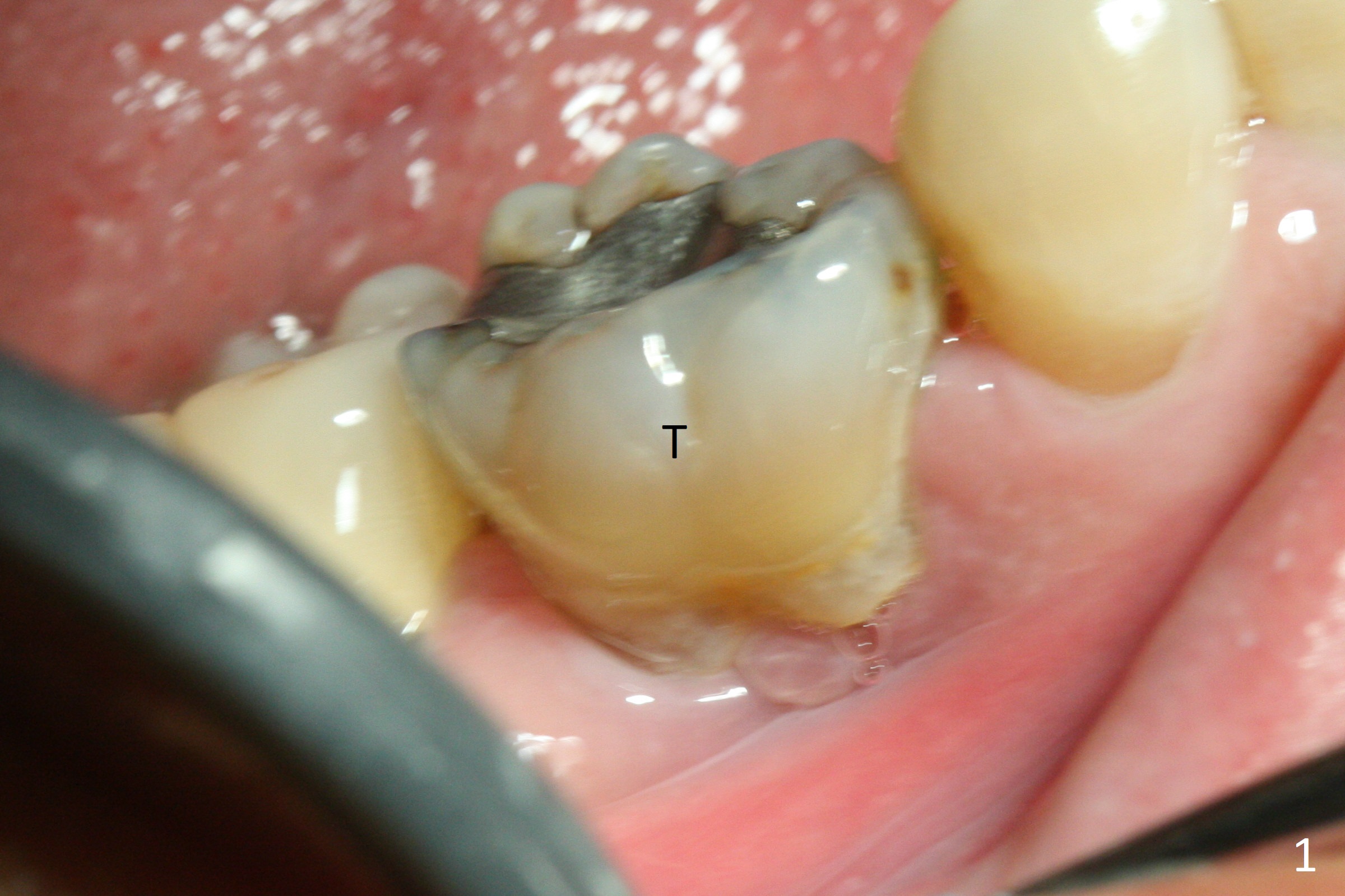
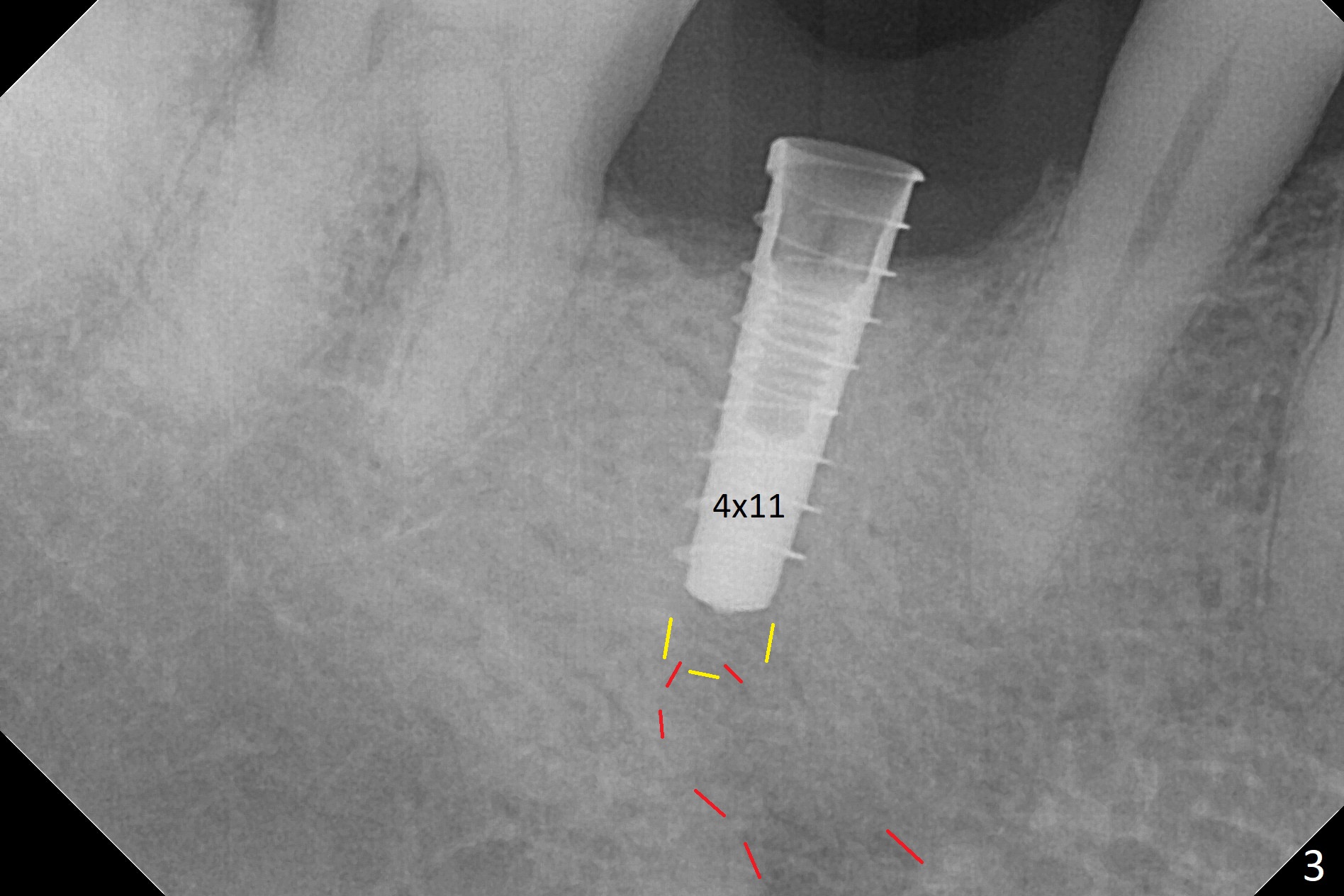
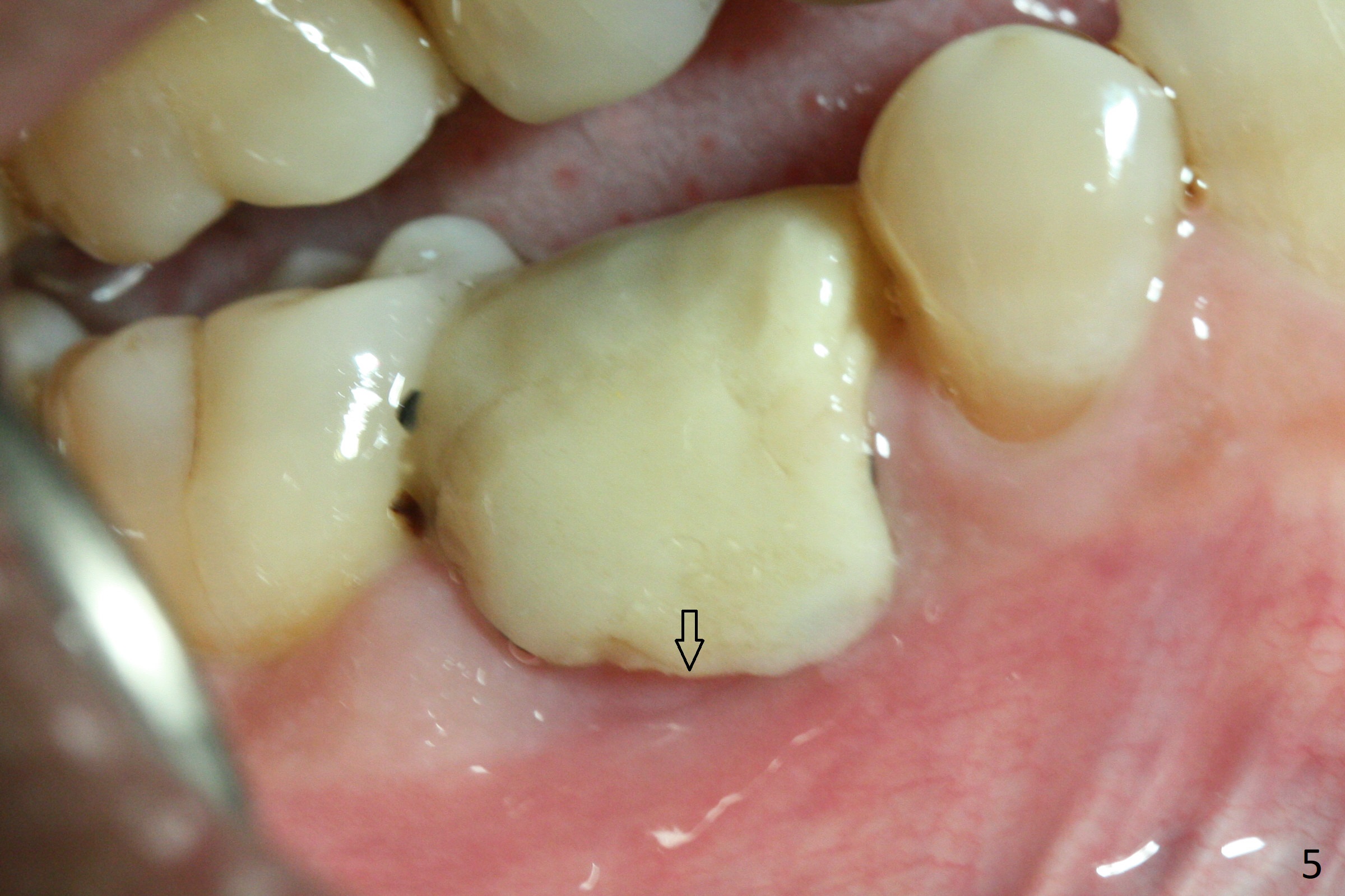
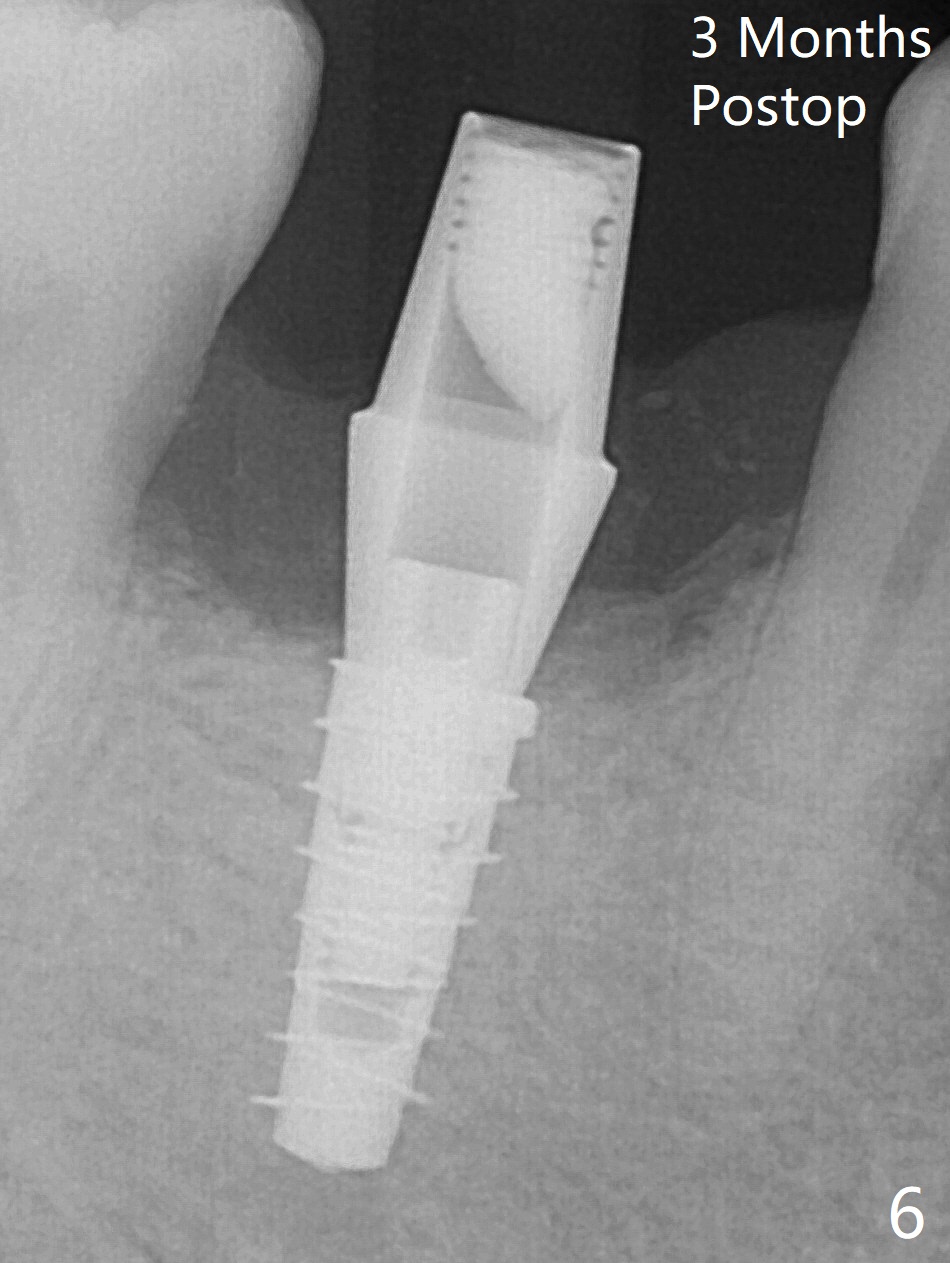
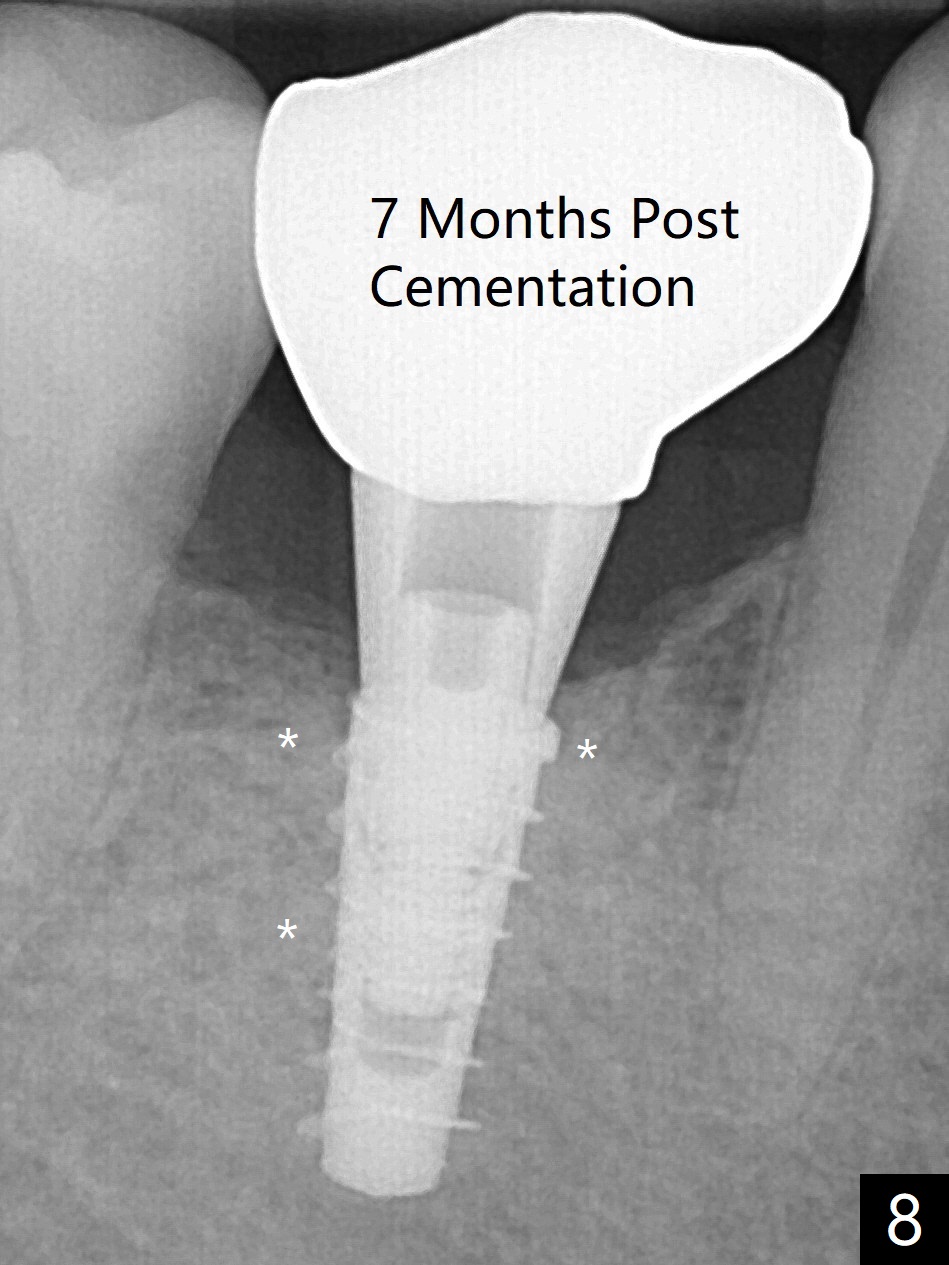
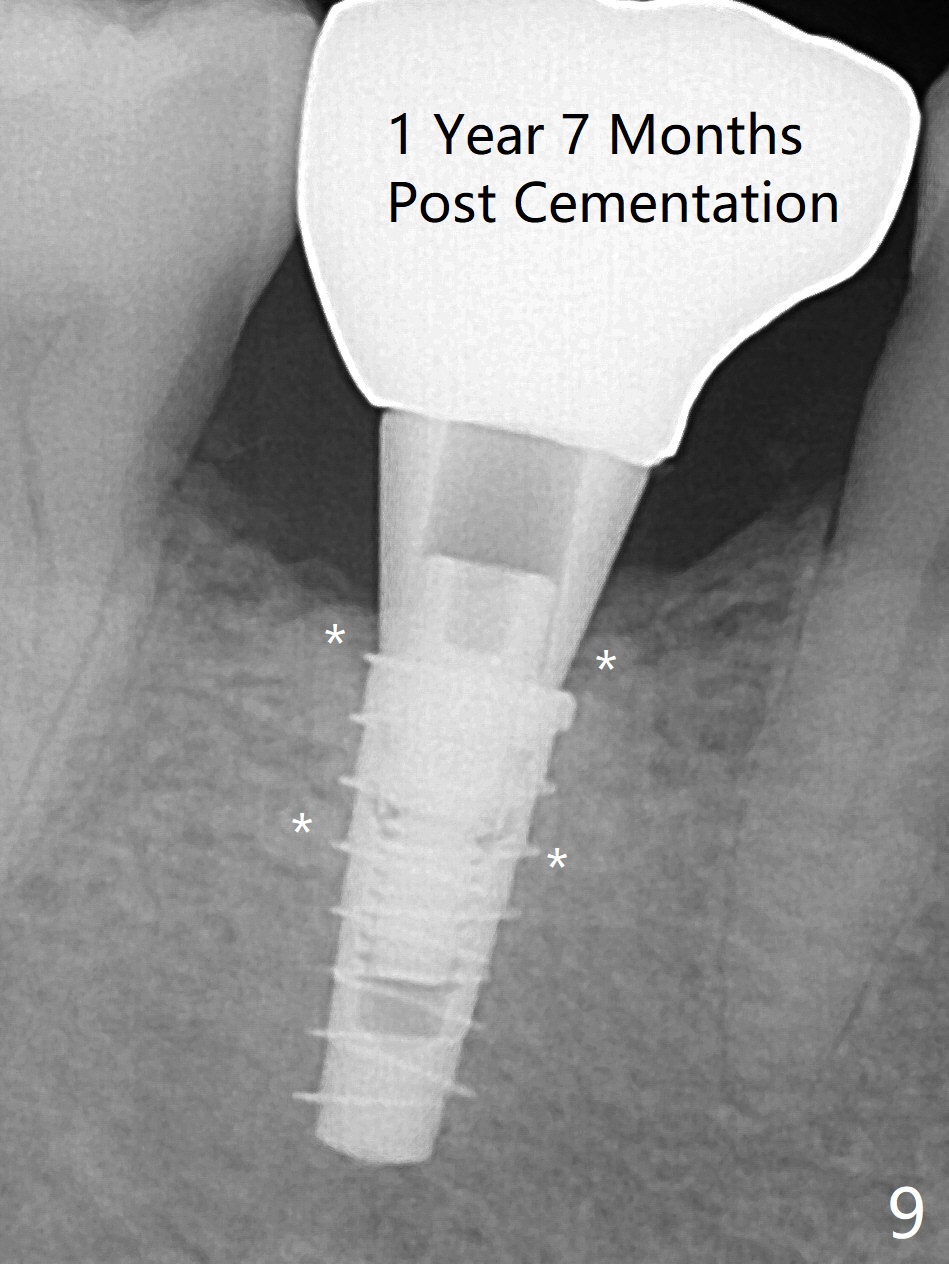
The retained deciduous tooth (lower right 2nd molar, Fig.1 T) has buccal apical infection and recession. After extraction, the initial depth of osteotomy is 11 mm over the flat socket bottom (Fig.2) without visible Mental Loop. Following 3.8 mm Magic Drill for 11 mm, a 4x11 mm dummy implant is placed partially due to hard bone; it appears that the apical osteotomy (Fig.3 yellow outline) overlaps the Mental Loop (red dashed line). For safety, a 4x9 mm IBS implant is placed with insertion torque 40 Ncm; a 5x5.7(4) mm abutment is immediately placed for an immediate provisional to cover the large socket and keep Vera graft in place (Fig.4 *). There is no postop paresthesia, probably due to the fact that the osteotomy is lingual to the Mental Loop. The provisional remains in place 7 days postop; its margin (Fig.5 arrow) covers the socket. The margin of the provisional is trimmed 1 month postop. Impression is taken nearly 3 months postop (Fig.6). The buccal plate looks atrophic 3 months postop (Fig.7 (immediately before cementation)), although there is no sign of periimplantitis. In the future, insert the immediate provisional inside of the buccal gingiva to make the buccal gingiva look bulky instead of buccal to it (Fig.5). The second drawback of placing an implant at the deciduous tooth area is that the crown is wide mesiodistally if orthodontic treatment is not rendered. Although there is lower anterior crowding, the patient declines orthodontic treatment. The bone density around the implant increases 7 months post cementation (Fig.8 *). The higher density bone seems to extend coronally 1 year 7 months post cementation (Fig.9). The dense bone apparently extends toward the abutment as well 3 years 5 months post cementation (Fig.10 curved arrows).
Return to Lower Primary Molar Immediate Implant Armaments Wife Xin Wei, DDS, PhD, MS 1st edition 11/15/2017, last revision 07/18/2021