





|
|
|
|
|
|
|
|
|
|
Every Step Should Have X-ray Confirmation
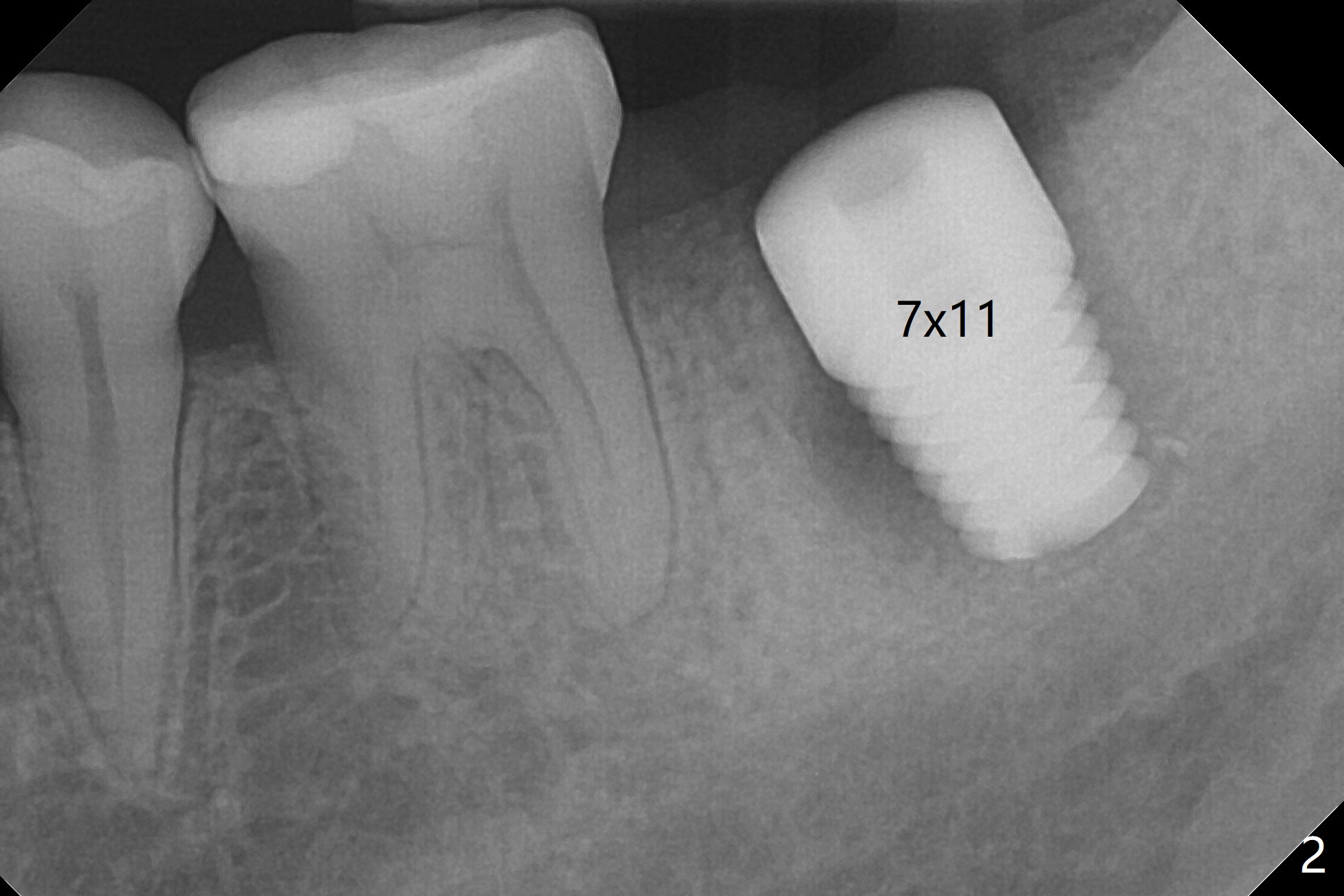
The patient with chronic buccal abscess at #31 is nervous. After extraction, a 7x11 mm tapered implant drops into the single socket, which is close to the Inferior Alveolar Canal (Fig.2). The bottom of the socket is sensitive to manipulation (explorer) after infiltration anesthesia. A 8x14 mm tapered tap is placed without binding, neither is a 8x14 mm cylindrical implant. The implant stability does not increase when Vera (.2-1.0 mm) or Vanilla (.5-1.0 mm) Graft is placed. Socket preservation is finished with Collagen plug and 6-month membrane (Fig.3,4).
If the patient were not nervous and every step were followed by X-ray, light osteotomy in the bottom of the socket (flattening) may increase primary stability. A larger implant (9 or 10 mm) is a solution. The socket heals with disappearance of the fistula 2 weeks postop (Fig.5,6), but the ridge seems to have been reduced in width. The patient return for follow up 4 months postop; bone graft appears to remain in the socket (Fig.7). The ridge is apparently reduced further (data not shown). The patient prefers to have implant placement 1 month later. Take photos of the ridge buccally when the patient returns. In fact the patient agrees to have guided surgery. She postpones the surgery due to sickness for one more month. Implant placement will occur 6 months post extraction. The bone density should be higher than earlier.
Return to Lower Molar Immediate Implant, Prevent Molar Periimplantitis (Protocols, Table), IBS, Another Cases, Upper 6th Meeting
Xin Wei, DDS, PhD, MS 1st edition 10/16/2017, last revision 09/12/2018