




|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Intraop Modification
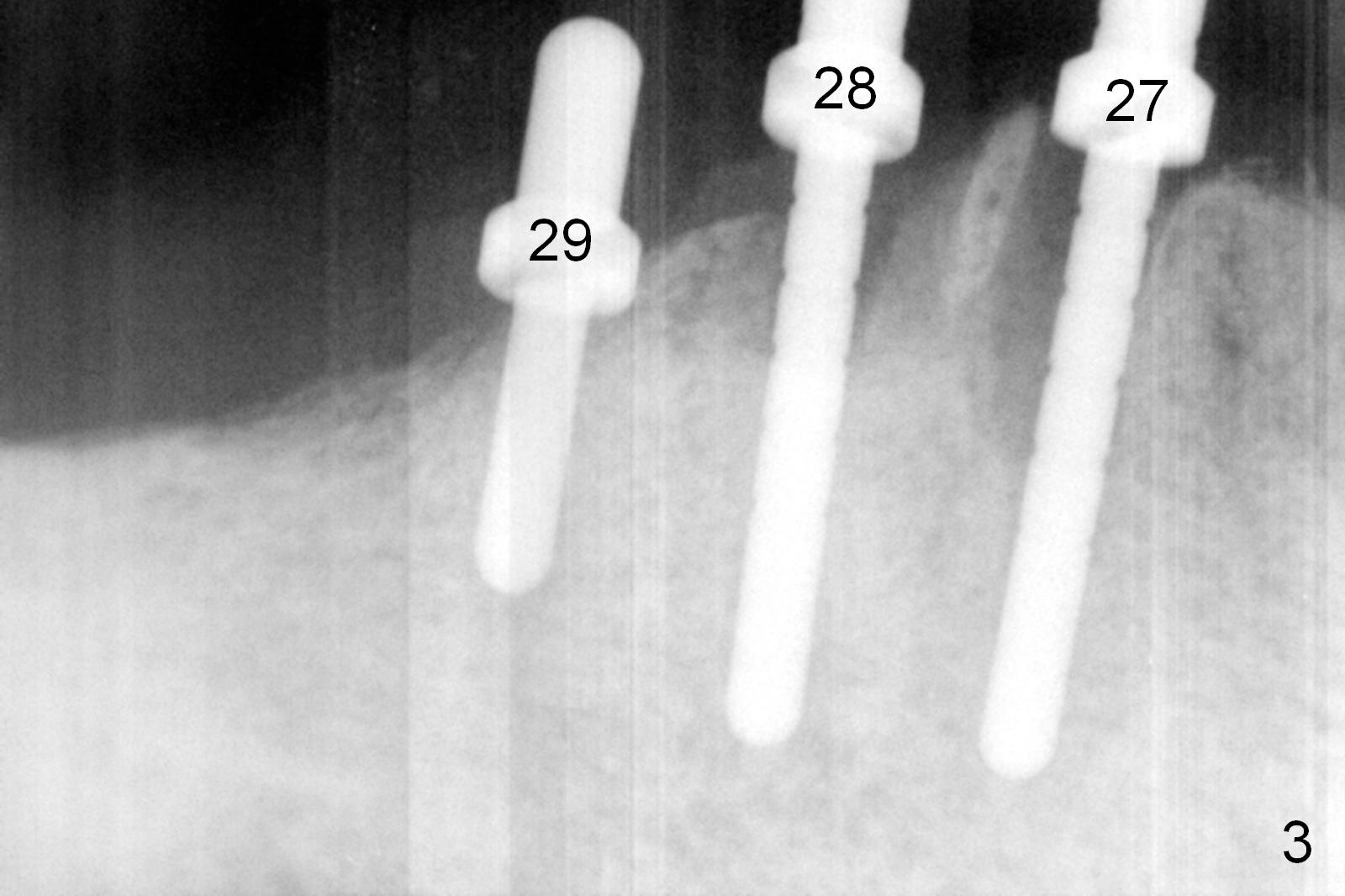
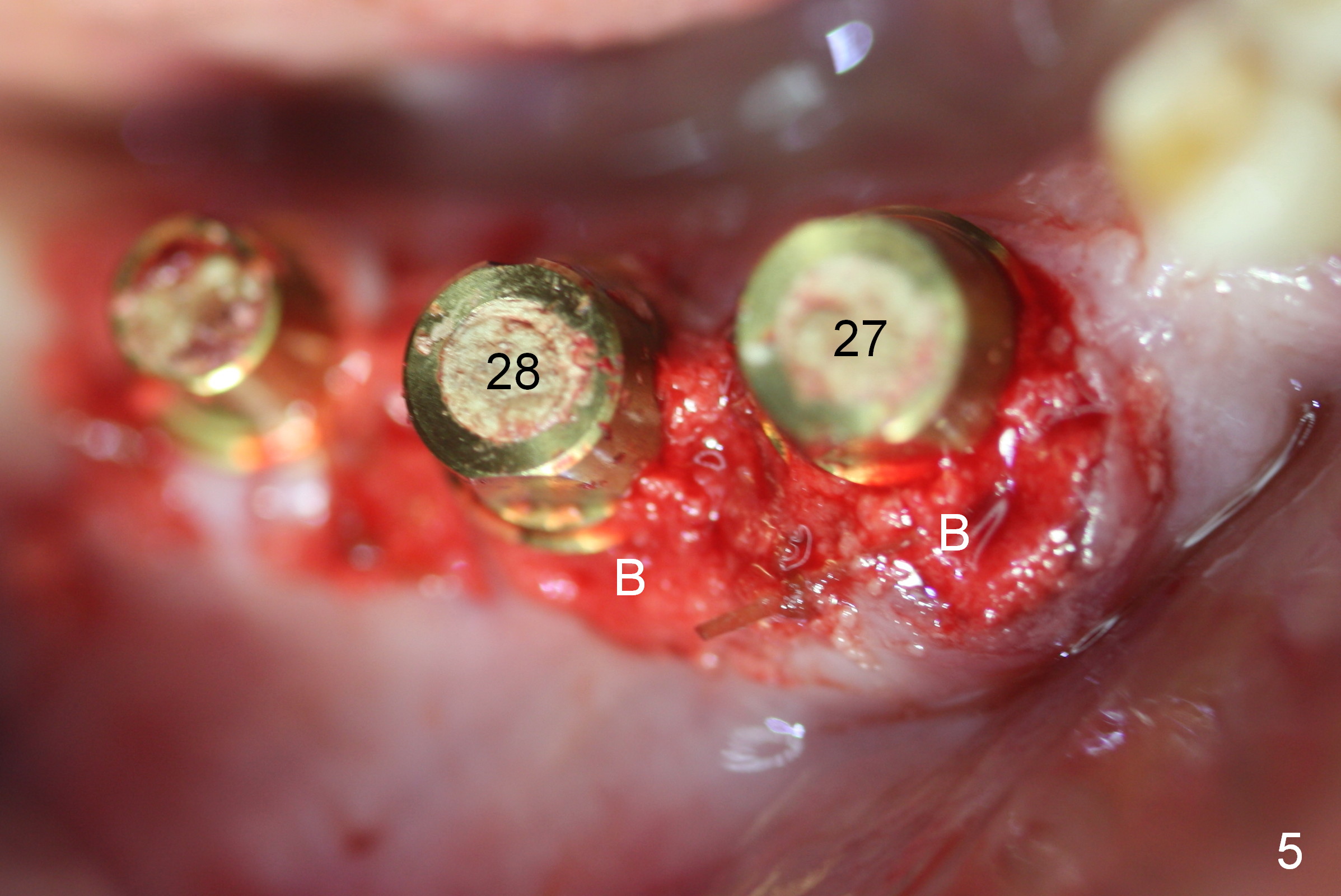
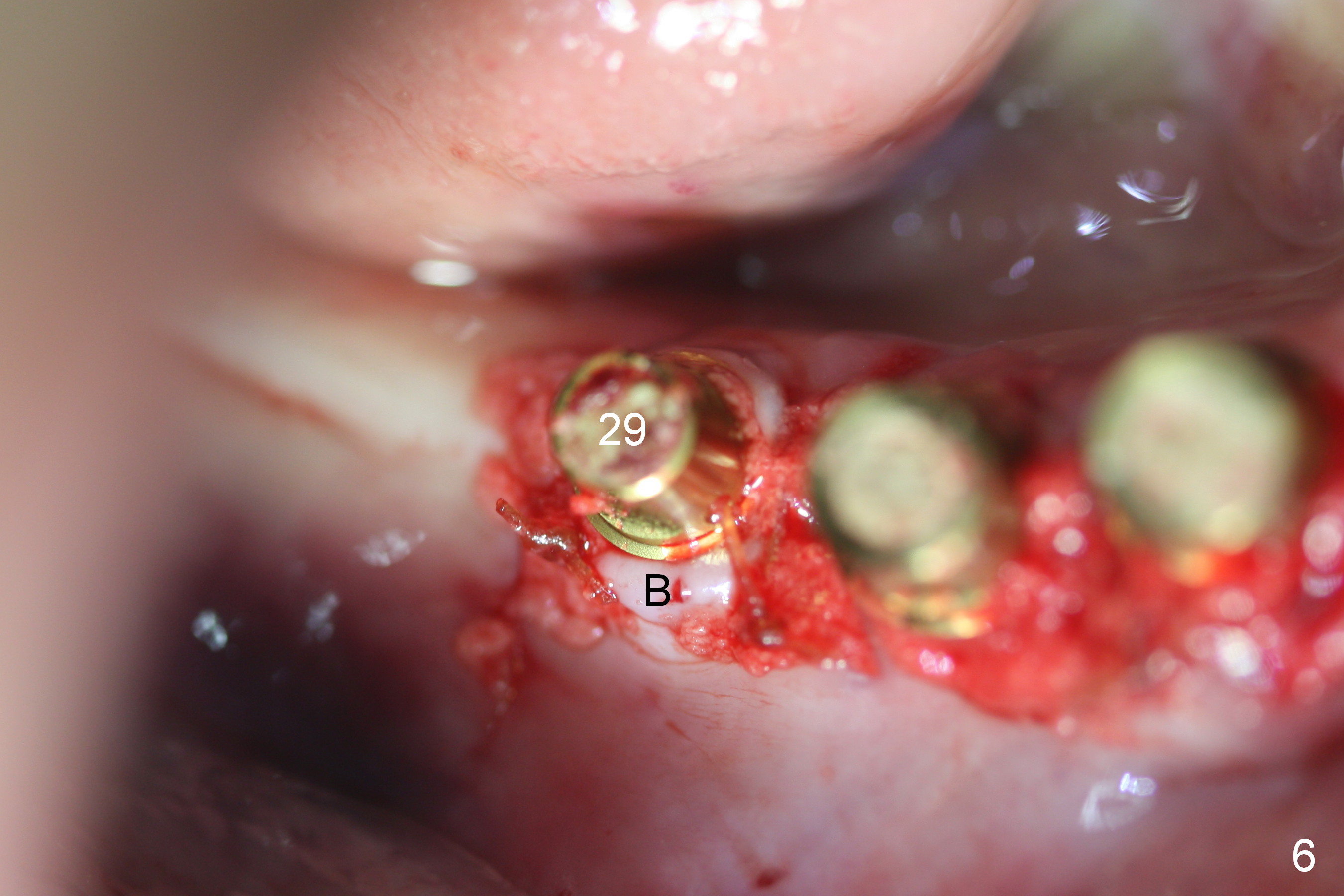
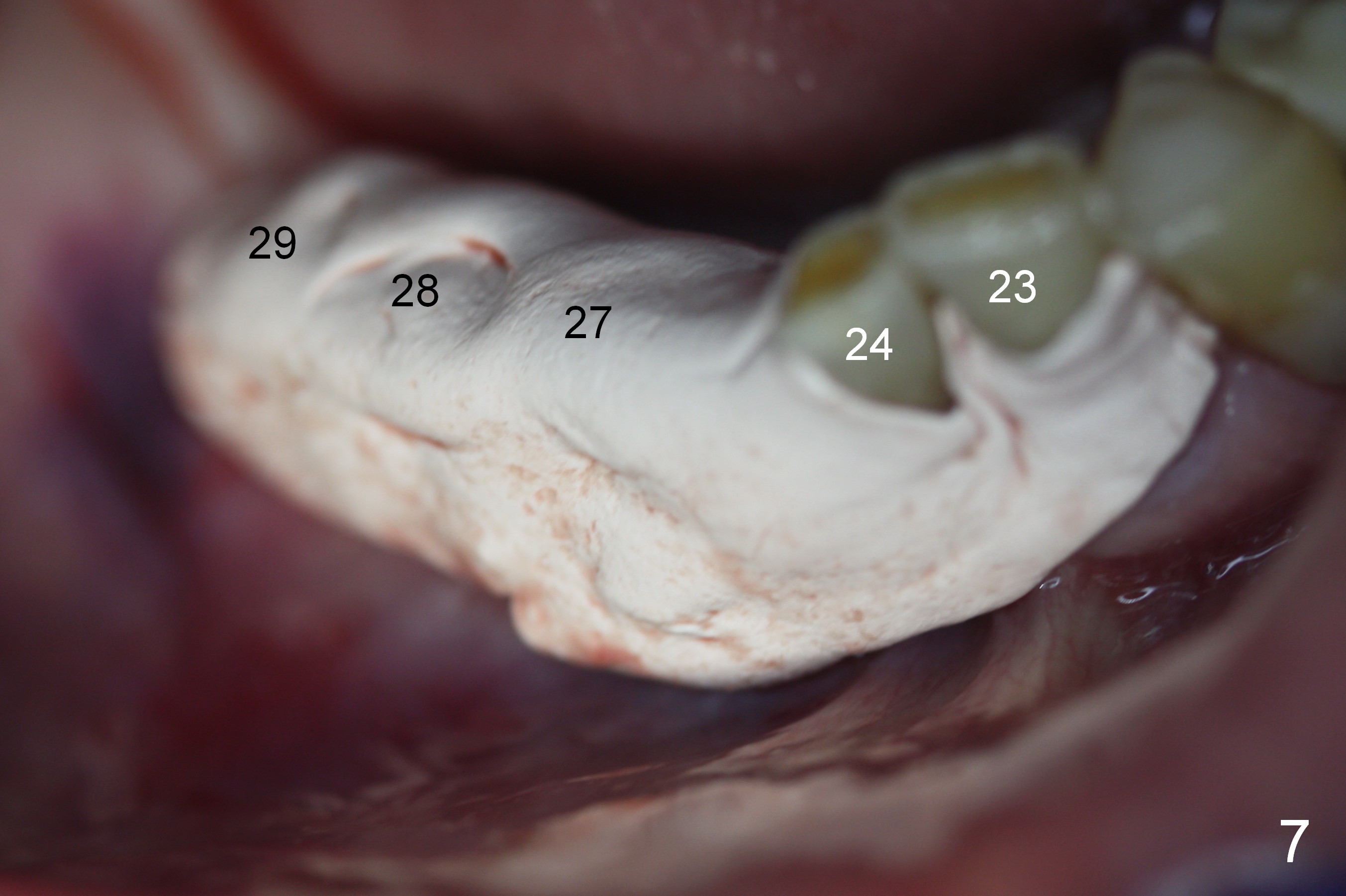
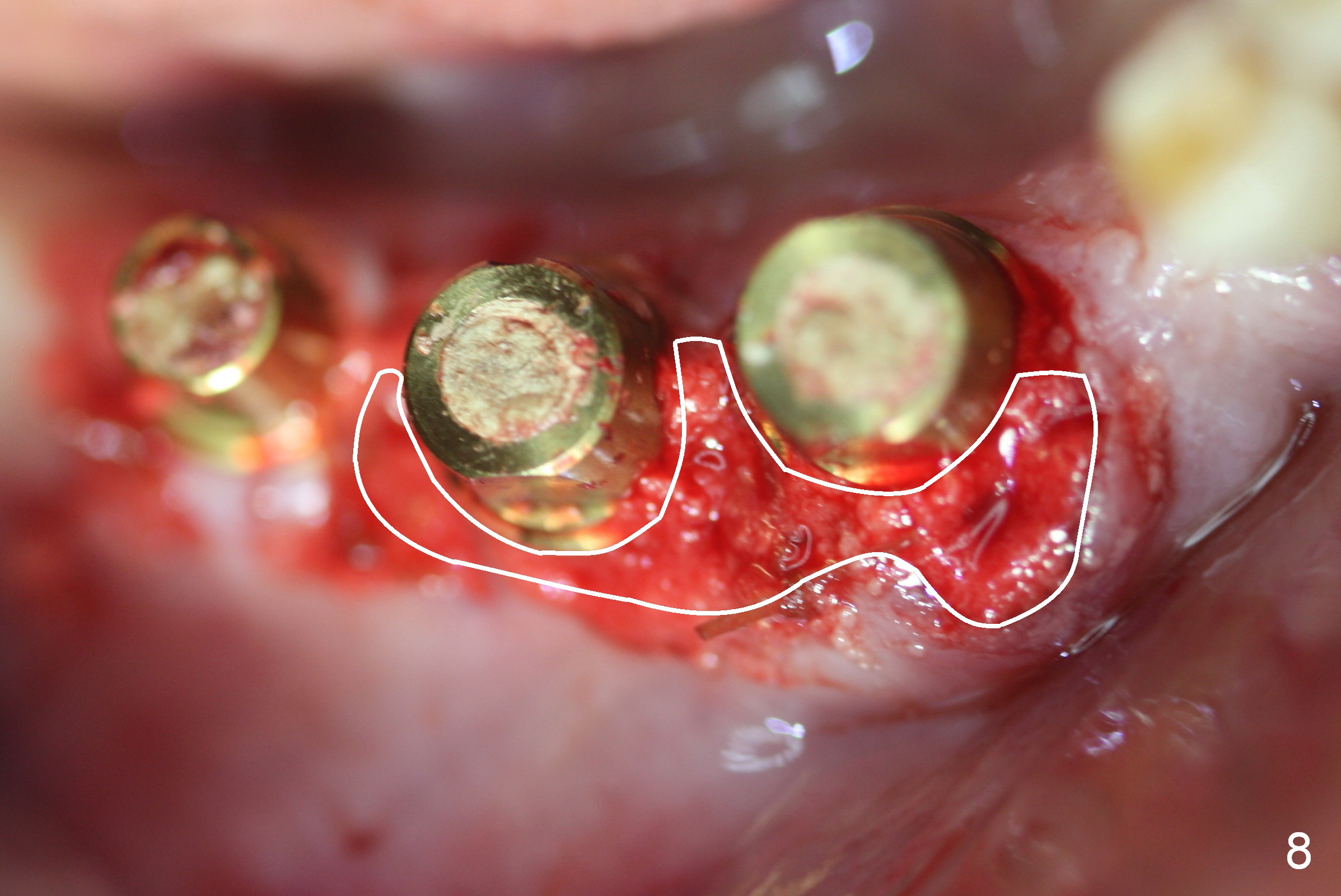
A 86-year-old man returns to office for the lower right quadrant reconstruction with implants. In addition to the immediate ones at the sites of #27 and 28 (Fig.1), how many and where else? The patient reveals that he does not plan to get an implant at the site of #3 (Fig.2). Therefore there is no need for an implant at #30. Preop CT shows that bone width is compromised at #26. So the 3rd site will be #29 (Fig.3,4). All of the 3 implants (4.5x14 mm, 4.5x12, and 4.1x12 mm) achieve primary stability (»55 Ncm). An immediate provisional could be provided, but it seems difficult to close the buccal (Fig.5 B) gaps of #27 and 28 after bone graft with the provisional. In contrast, the gingiva adapts to the implant at #29 well (Fig.6 B). Perio dressing is applied to the abutments (Fig. 7: #27-29), the edentulous space at #26 and the neighboring teeth (#23,24). It would be ideal to apply a non-resorbable membrane to the buccal opening at #27,28 (Fig.8 white line) prior to perio dressing placement. In case of dislodgement of the latter, the membrane is able to keep bone graft in place.
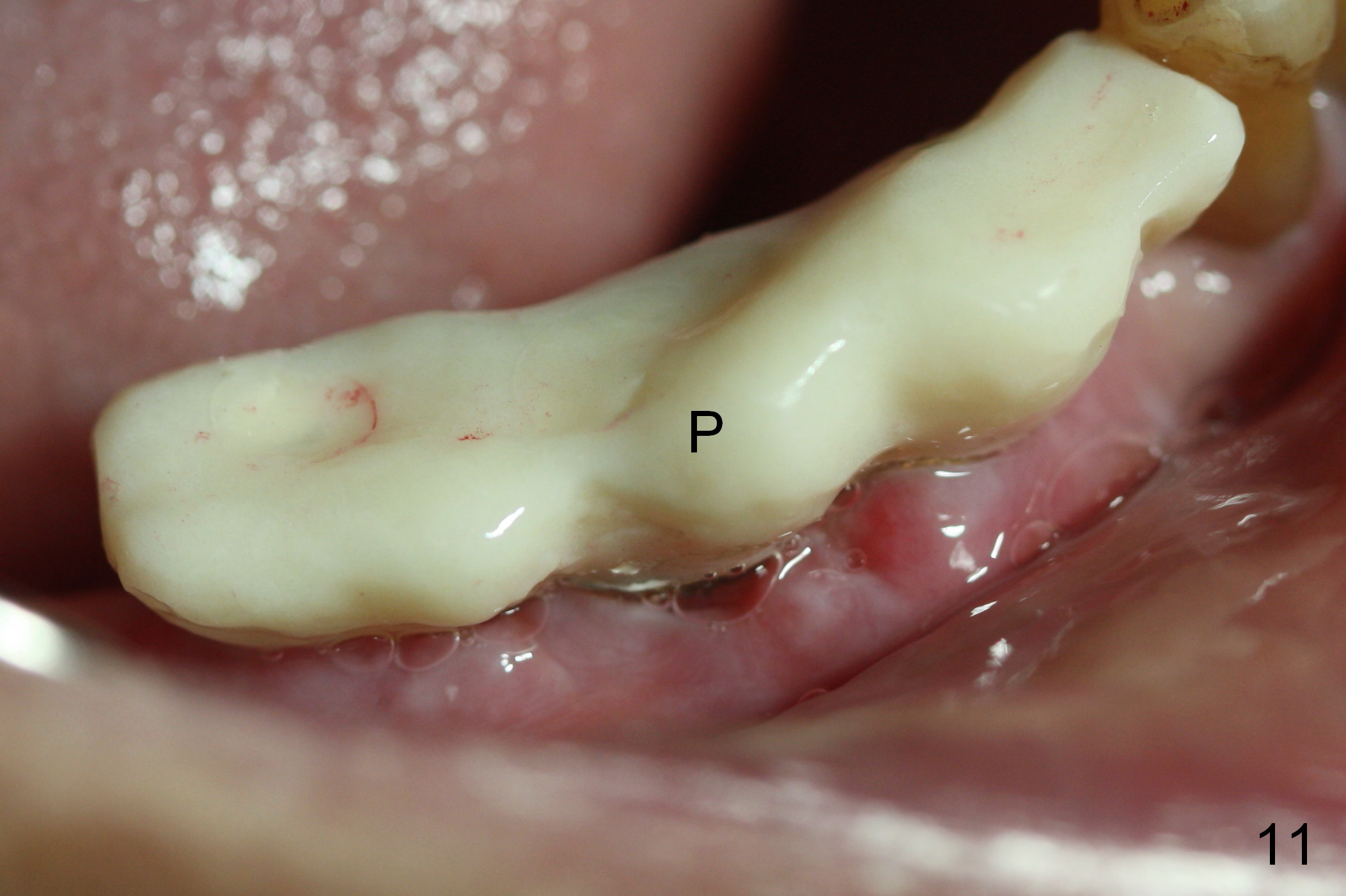
Eight days postop, the most anterior portion of the perio dressing is dislodged; the rest is stable (Fig.9). Since the patient has difficulty in coming to office, the perio dressing is removed. While the buccal gap of #27 has closed apparently (Fig.10 ^), that of #28 not (*). To prevent irritation from the abutments, a splinted provisional is fabricated (Fig.11 P). Perio dressing should have been re-applied buccal to the gap at the site of #28 or preferably the original perio dressing should have not been removed prematurely.
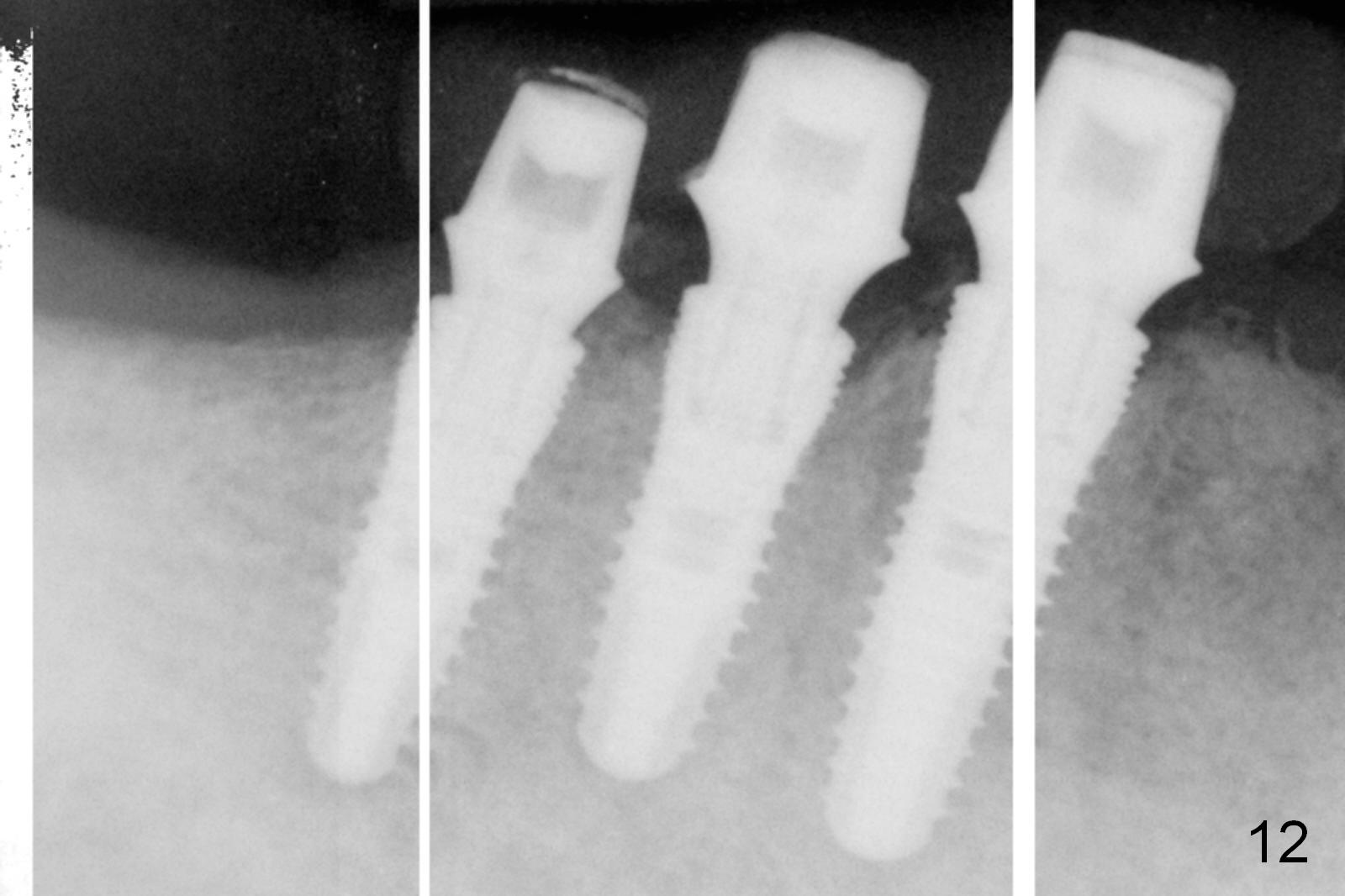
The patient returns for definitive restoration 5 months postop. There is no gross bone resorption around the implants (Fig.12). The surrounding gingiva is healthy (Fig.13). Since the edentulous space at #26 is relatively wide, one option is to splint #26-28 with #29 single. If the abutments at #27 and 28 are not parallel and the gingival margins are not at the same level too much, simply splint #26 and 27, since the implant at #27 is relatively long and wide.
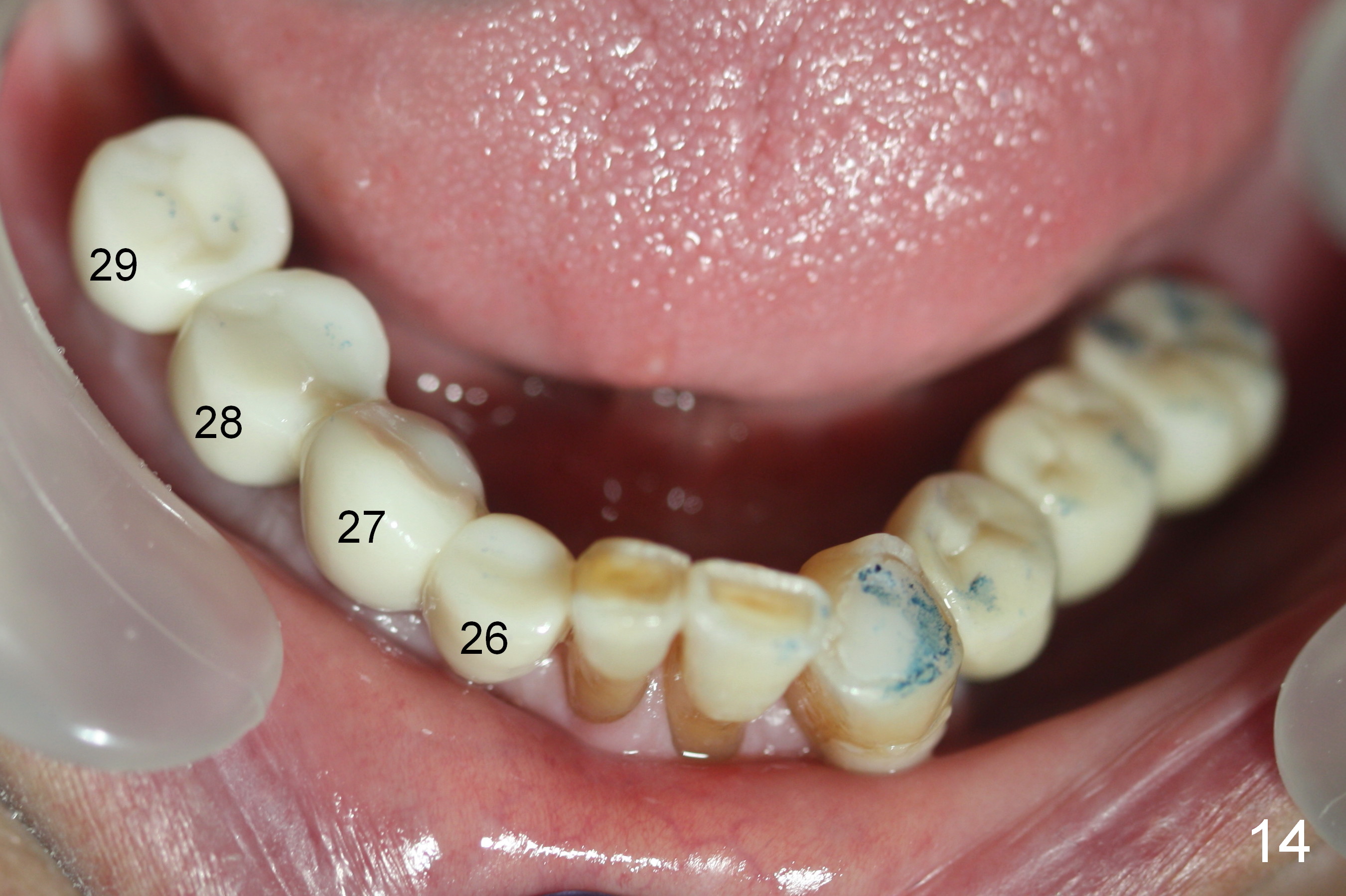
In fact, the crowns are splinted between #26-28, while the one at #29 is single unit (Fig.14). The patient is concerned that the bite on the lower right side is not strong. The occlusion for the most distal crowns should be tight.
Return to Lower Full Arch
Reconstruction,
Posterior Immediate Provisional,
Technicians,
14
Xin Wei, DDS, PhD, MS 1st edition 08/20/2015, last revision 11/08/2017