
,%20native%20bone%204.8%20mm.jpg)
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
2-Pointed Fixation
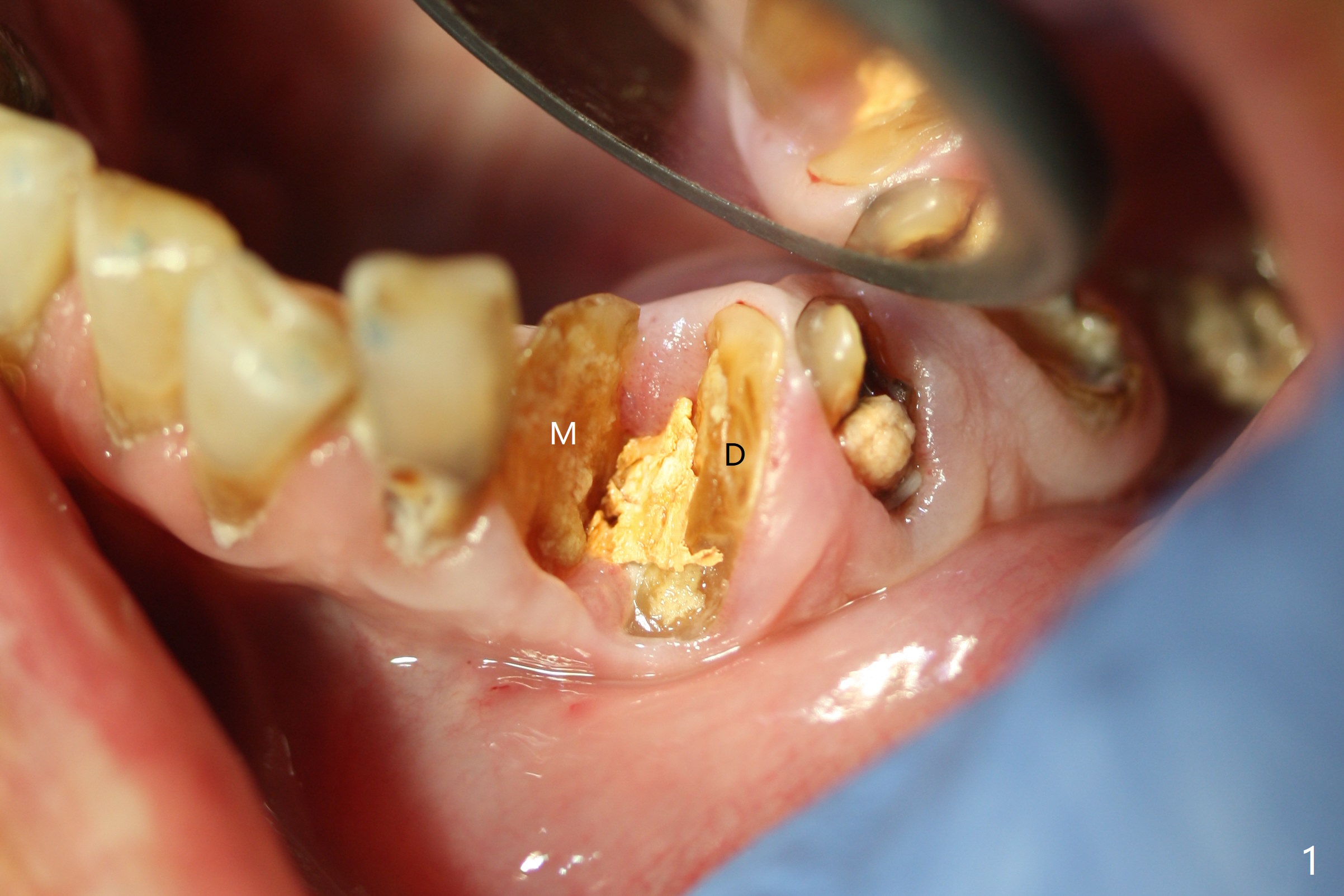
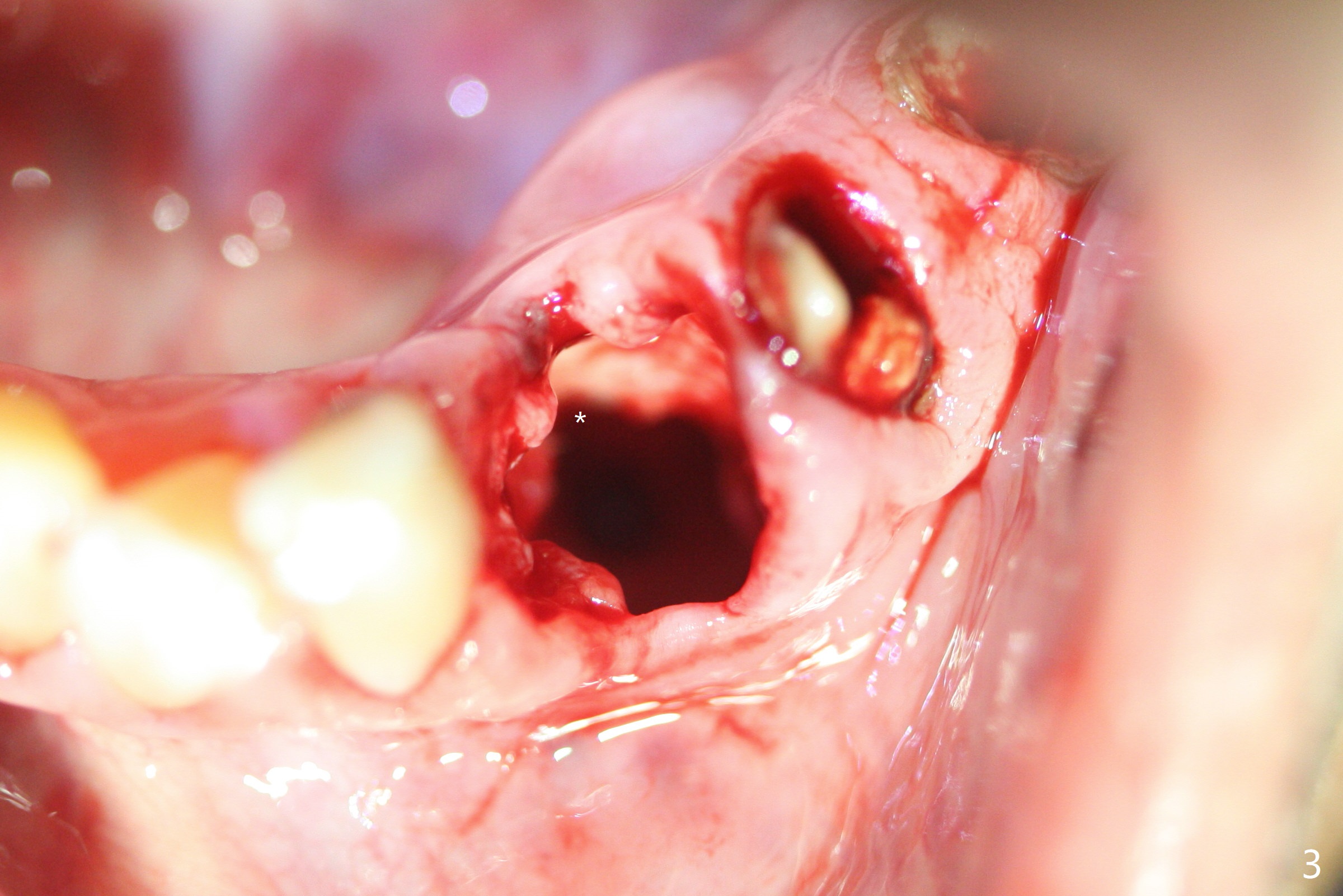
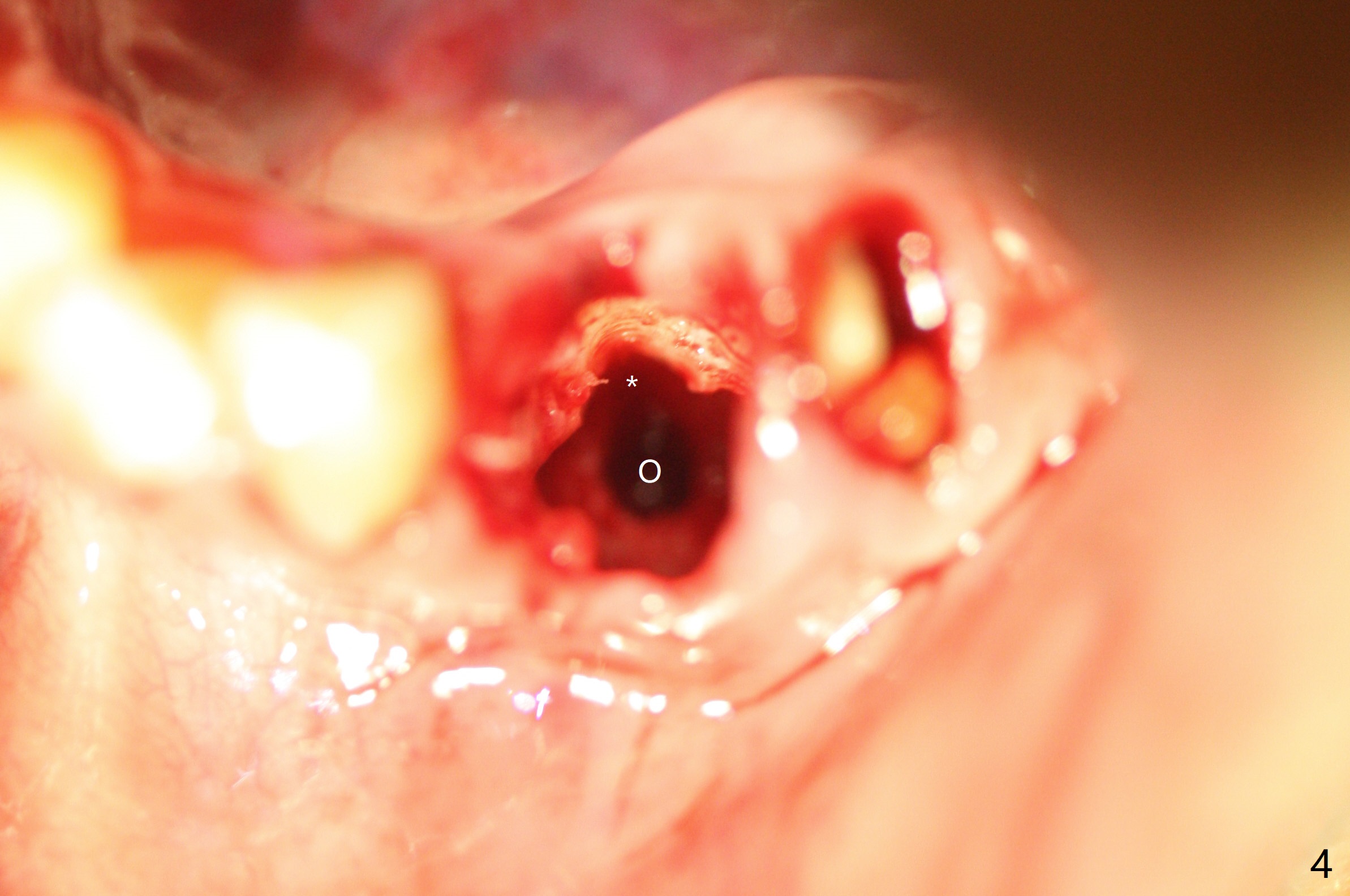
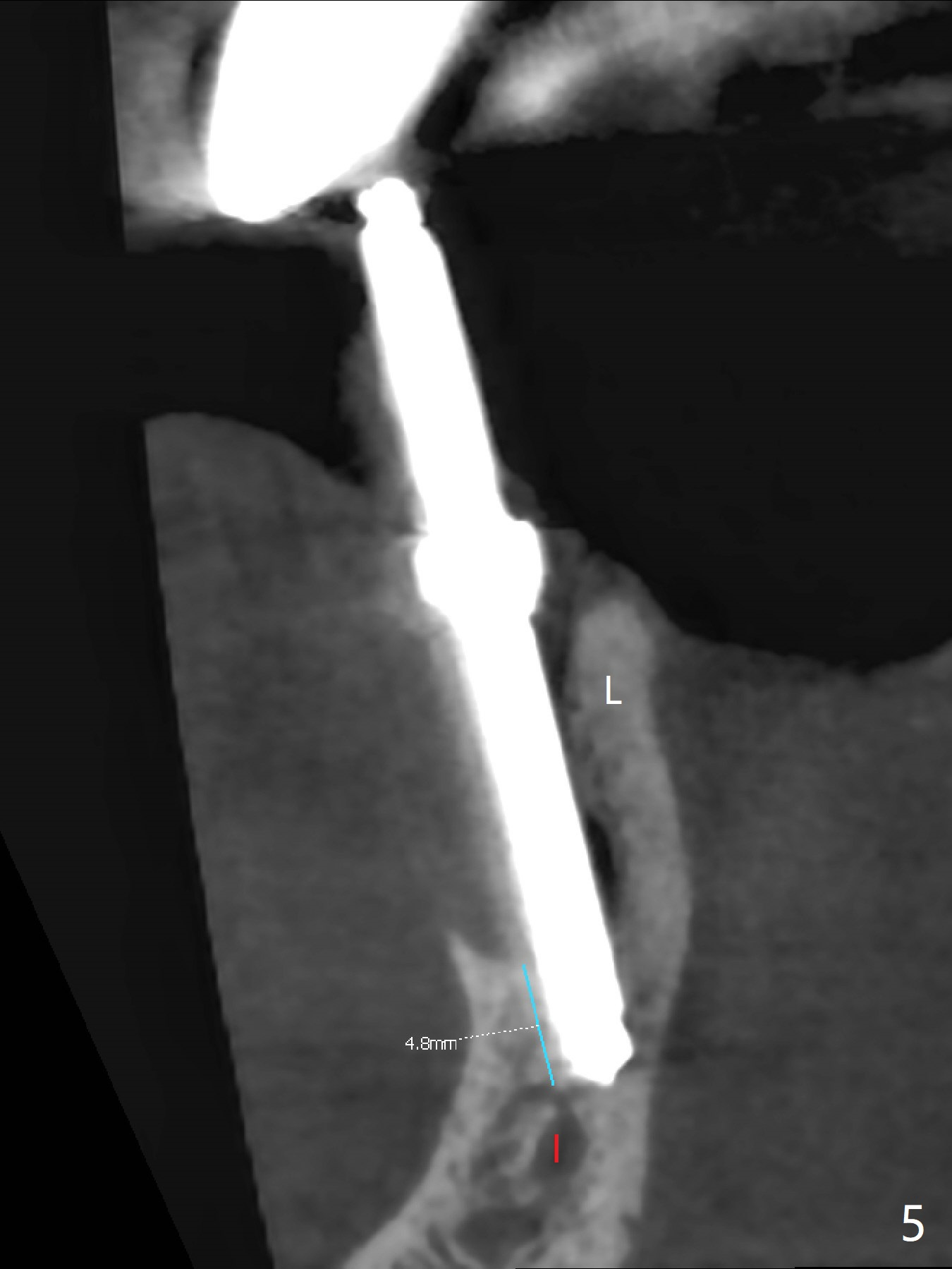
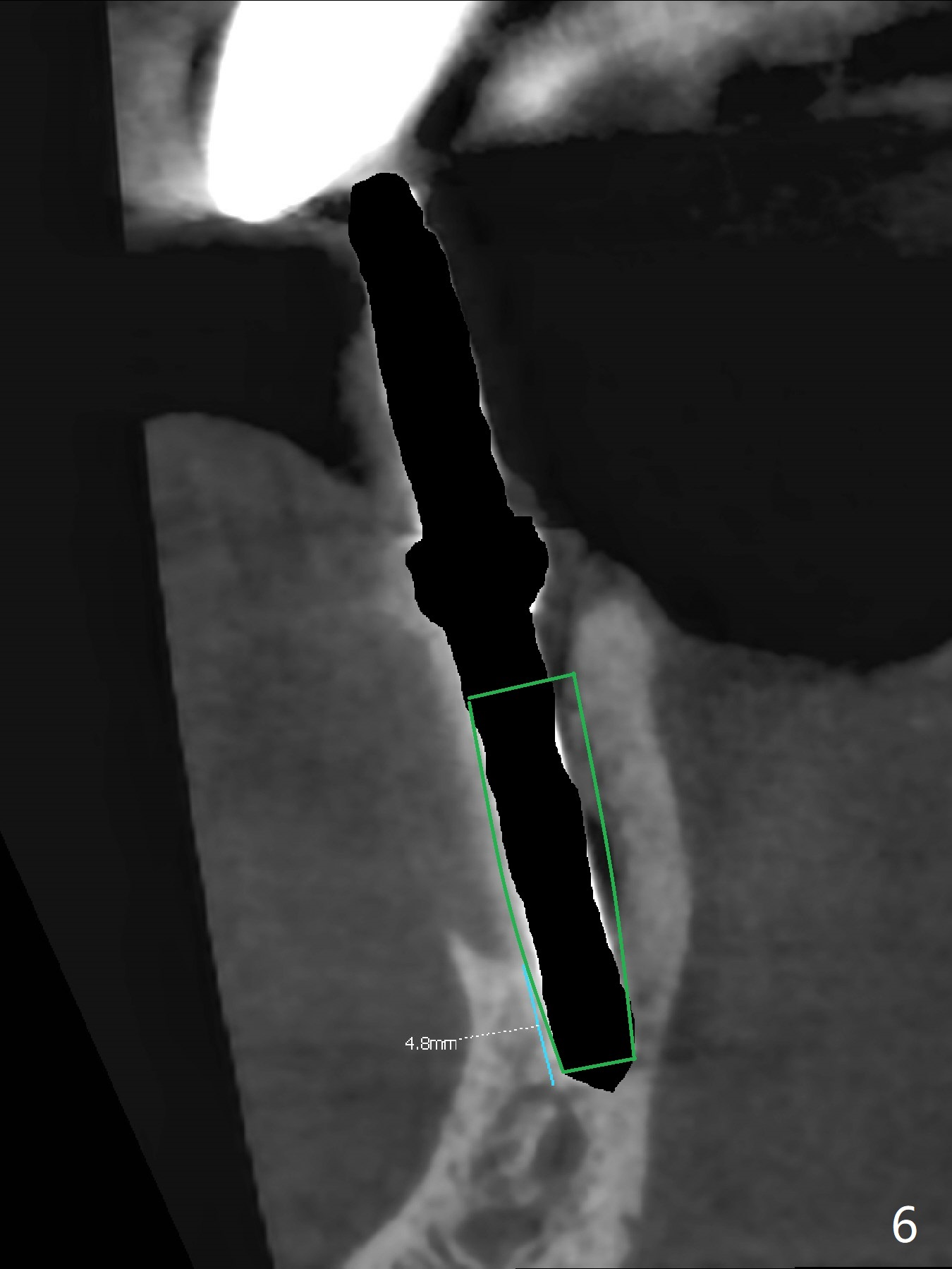
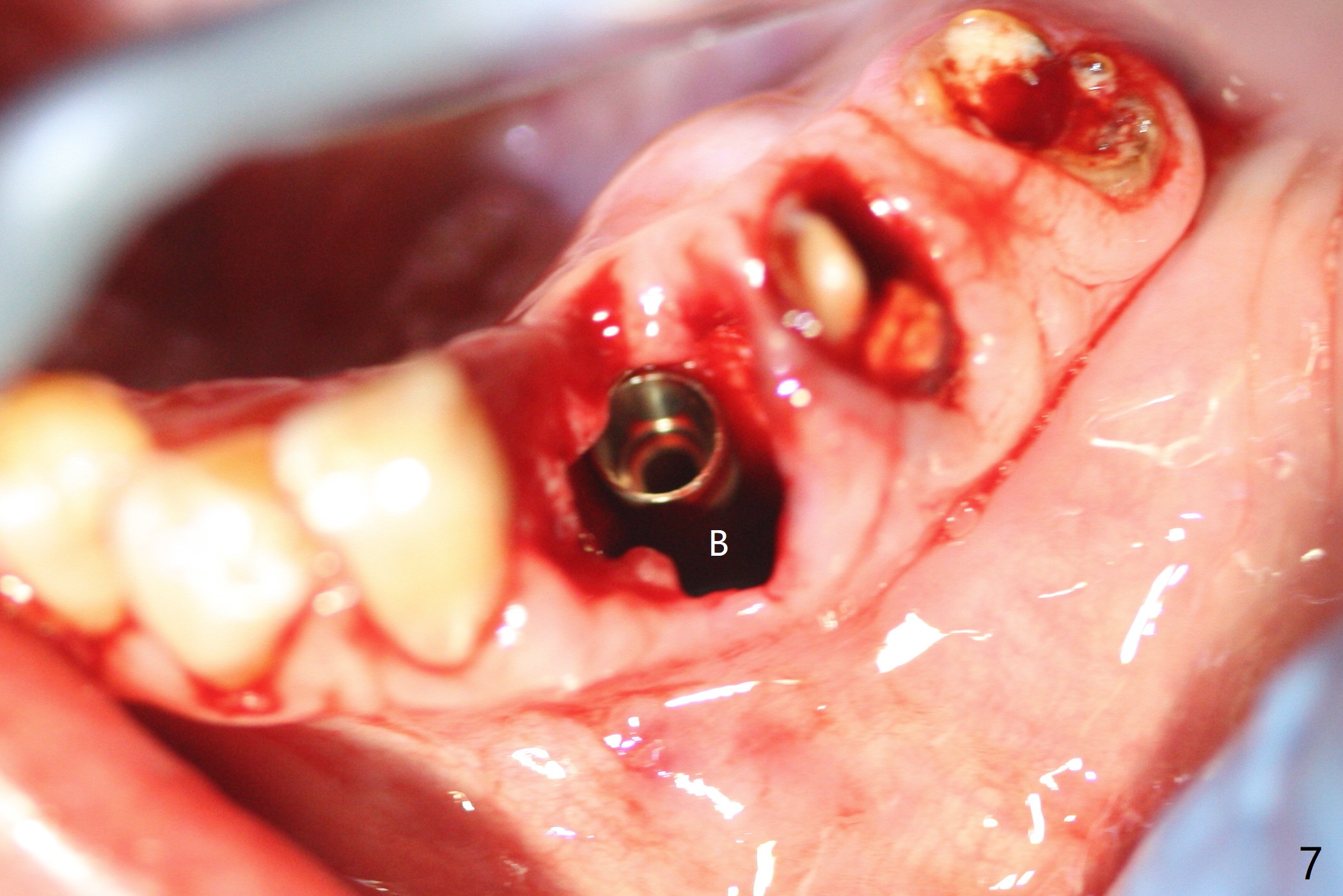
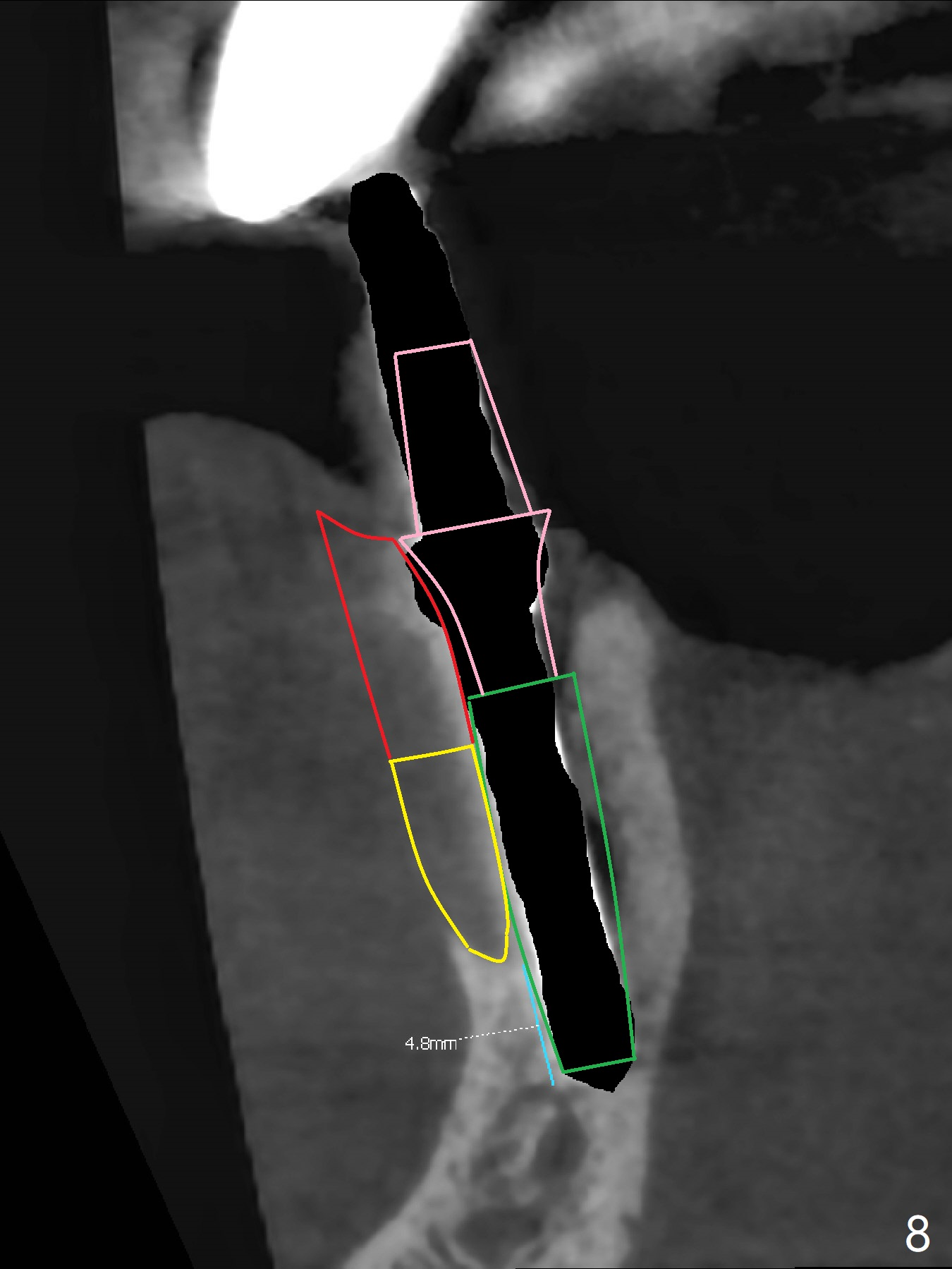
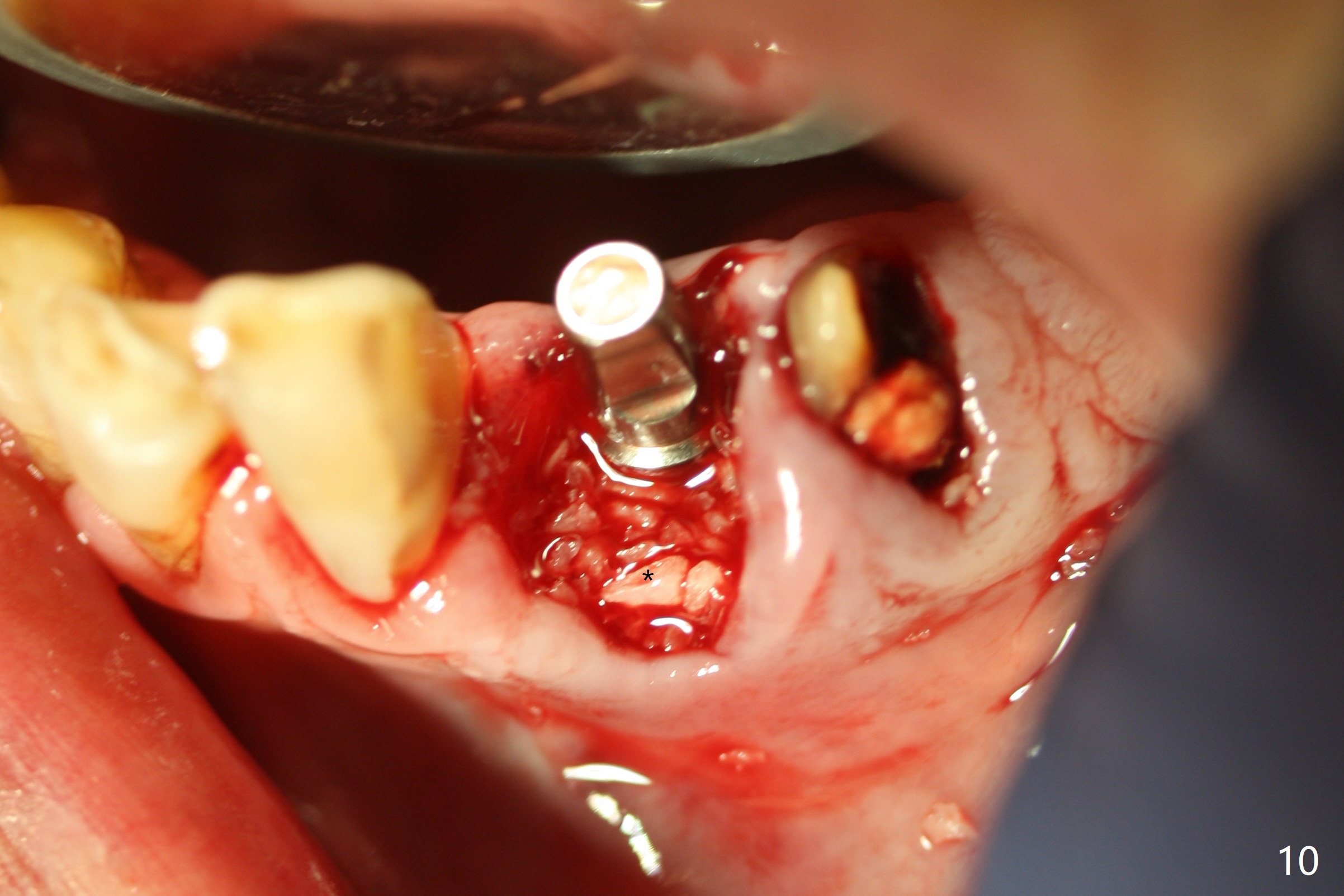
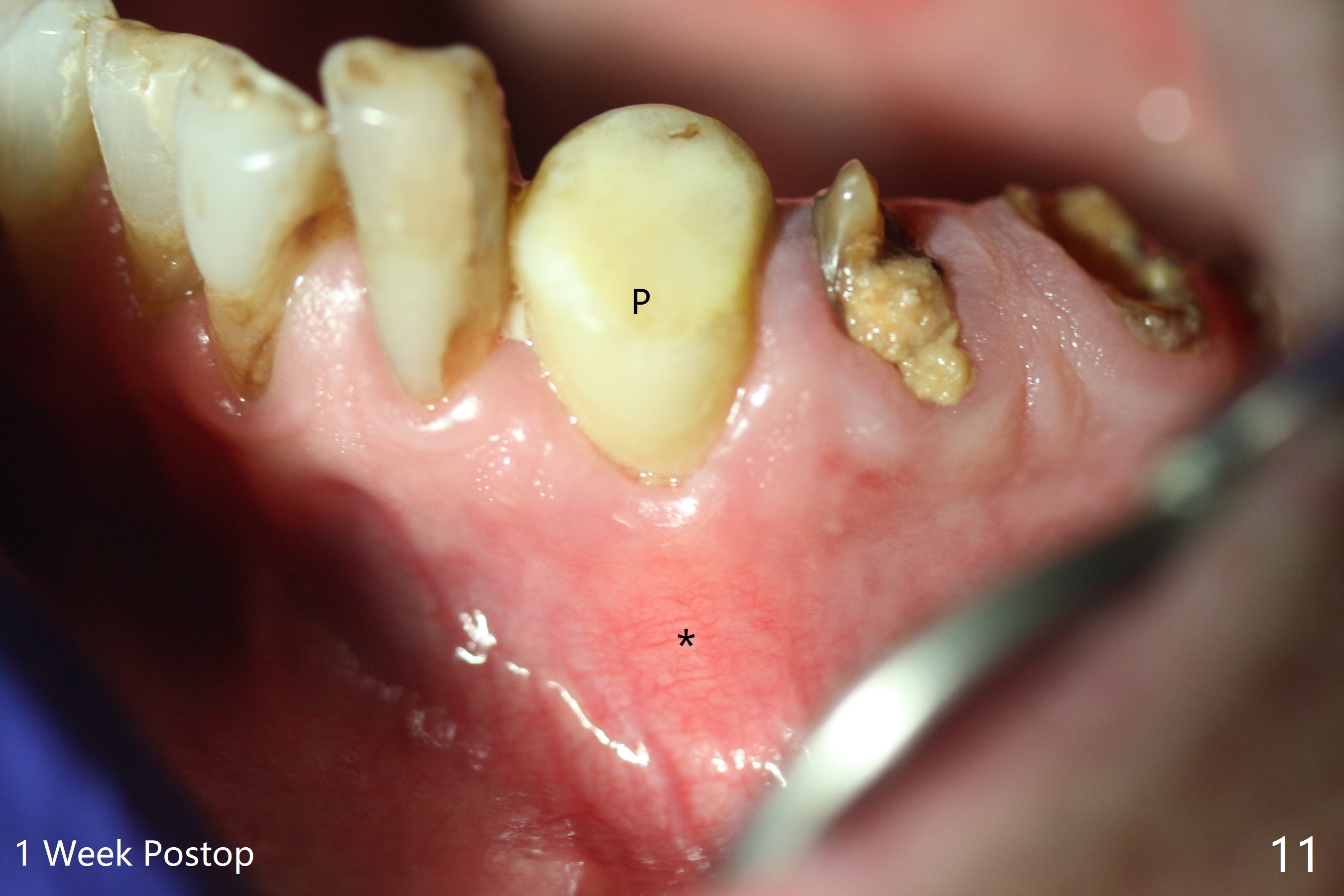
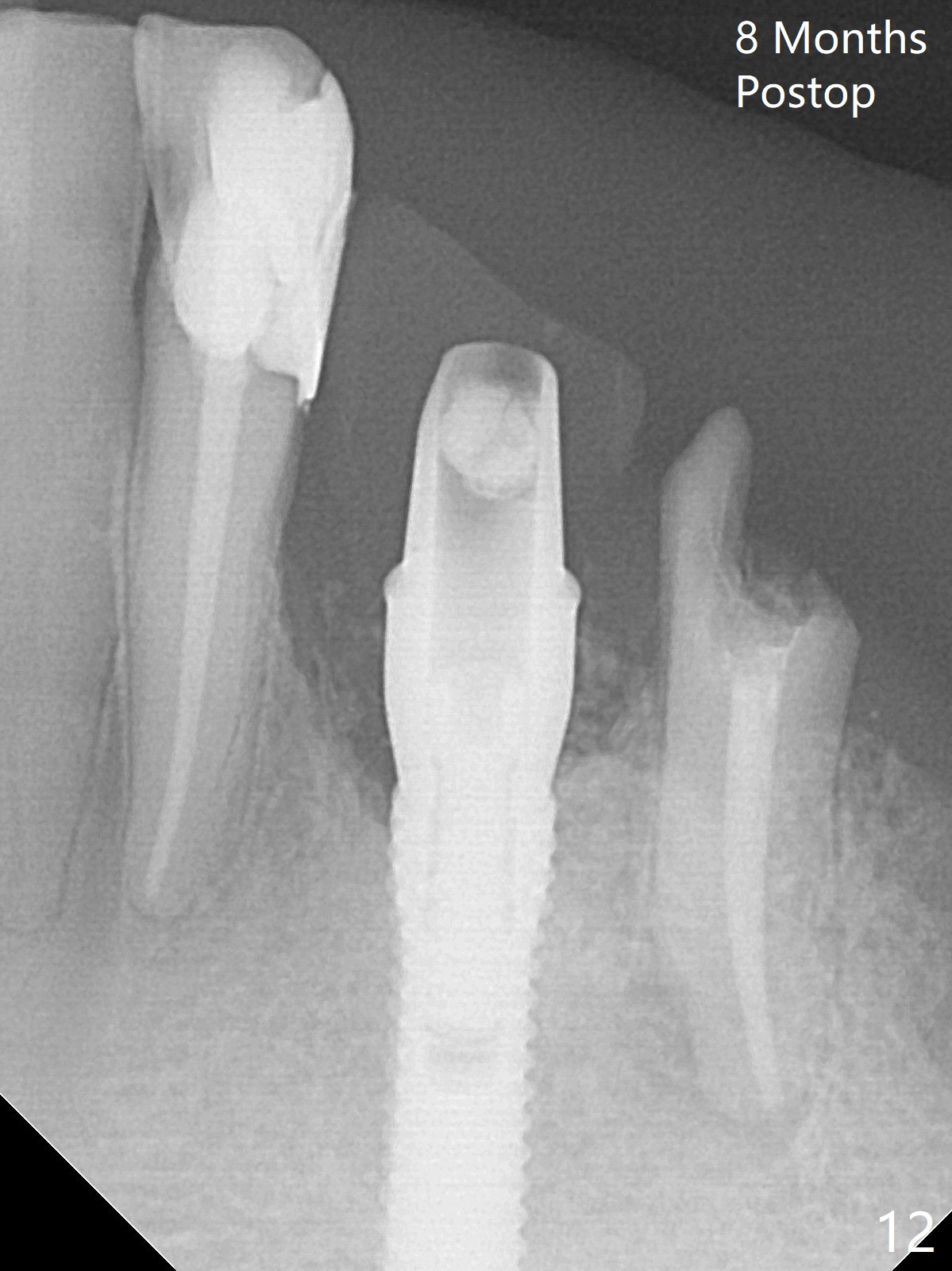
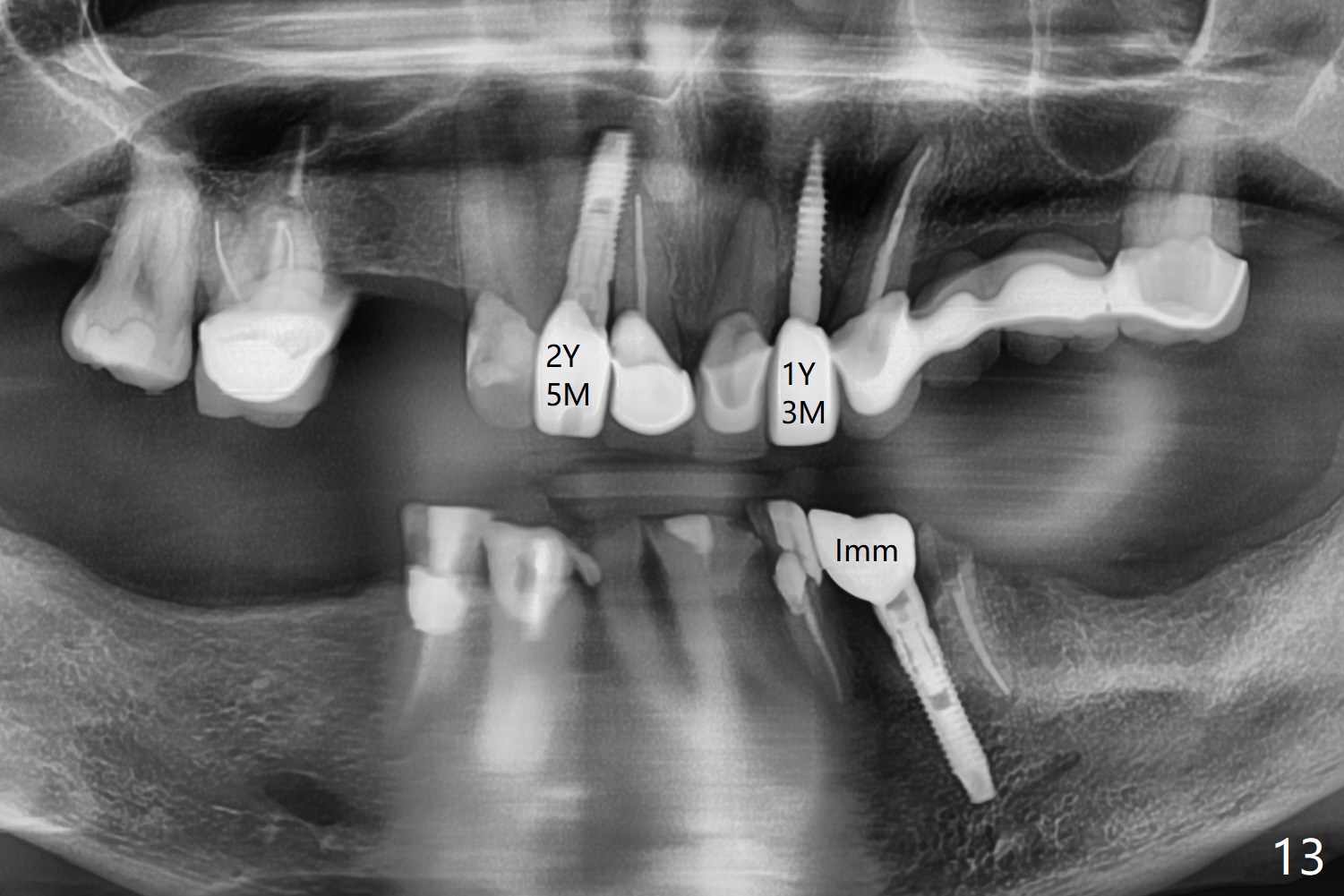
After removal of the split residual roots at #22 (Fig.1), the buccal wall is found to be defective, while the coronal portion of the lingual one (Fig.2 L) is confirmed to be more buccal than the apical portion. A vertical slot is made in the coronal portion of the lingual plate (Fig.3 *) in order to establish osteotomy lingual (Fig.4 O). The depth of the osteotomy in the apical native bone is 4.8 mm (Fig.5 CT coronal section). After the final drill (3 mm) is removed, a 3.8x16 mm implant is placed lingually for secure 2-pointed fixation (Fig.6,7, coronally: mesiolinguodistal; apically: in the native bone (Fig.9)). The essence of the lingual placement is the presence of a large buccal gap for Osteogen plug (Fig.8 yellow) and allograft (Fig.8 red, 9,10 (*)) for potential regeneration of the buccal plate. With bone graft and the overlying provisional (Fig.11 P), the buccal plate seems to have been established (*) 1 week postop. There is no obvious implant thread exposure 8 months postop (Fig.12). But the buccal plate is atrophic when the crown is cemented (~10 months postop, Fig.13).
Return to
Lower Canine
Immediate Implant,
Trajectory 7
10
Xin Wei, DDS, PhD, MS 1st edition
01/10/2019, last revision
11/06/2019
,