



|
|
|
|
|
|||
|
|
|
|
|
|||
|
|
|
|
||||
|
|
|
|
|
|||
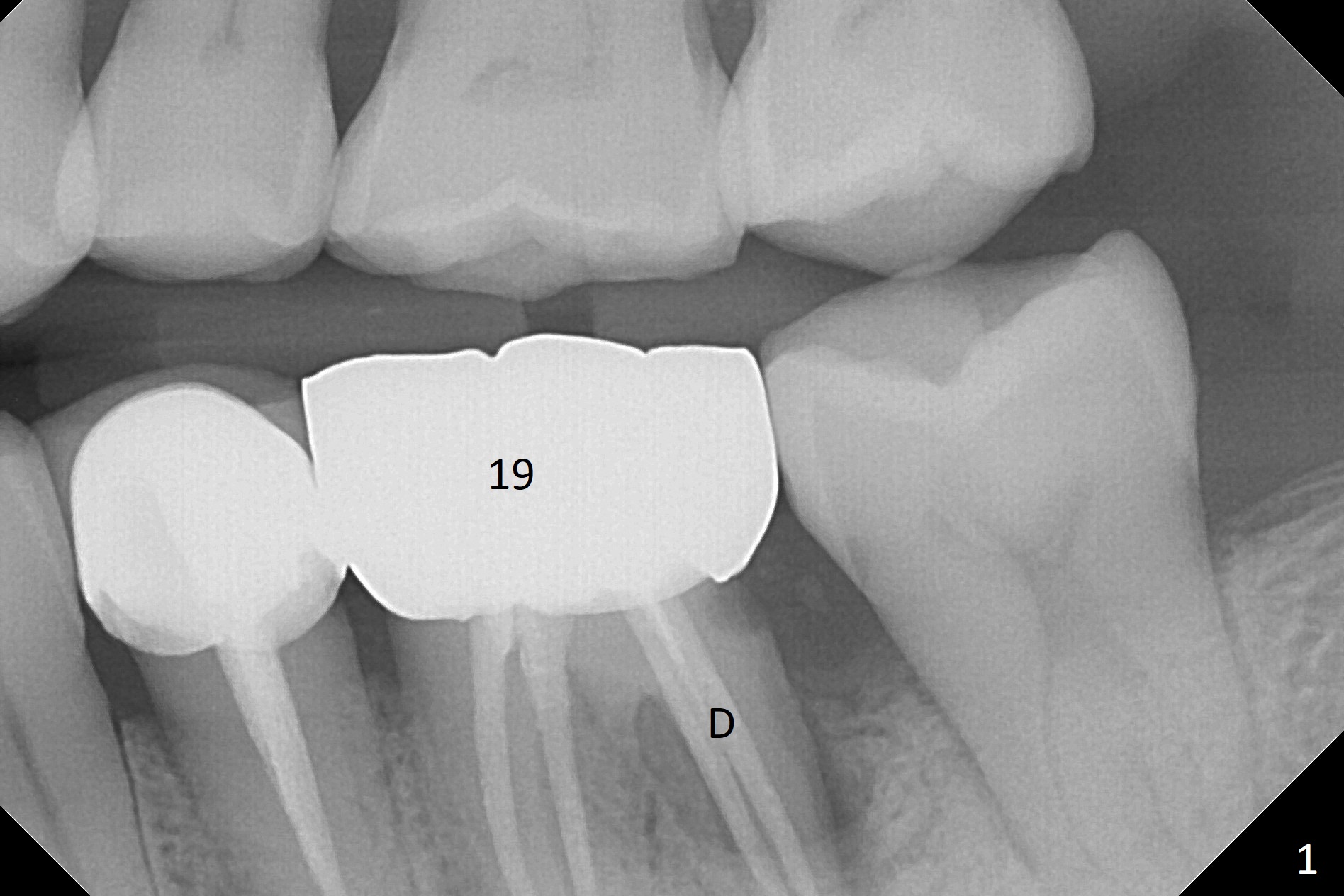
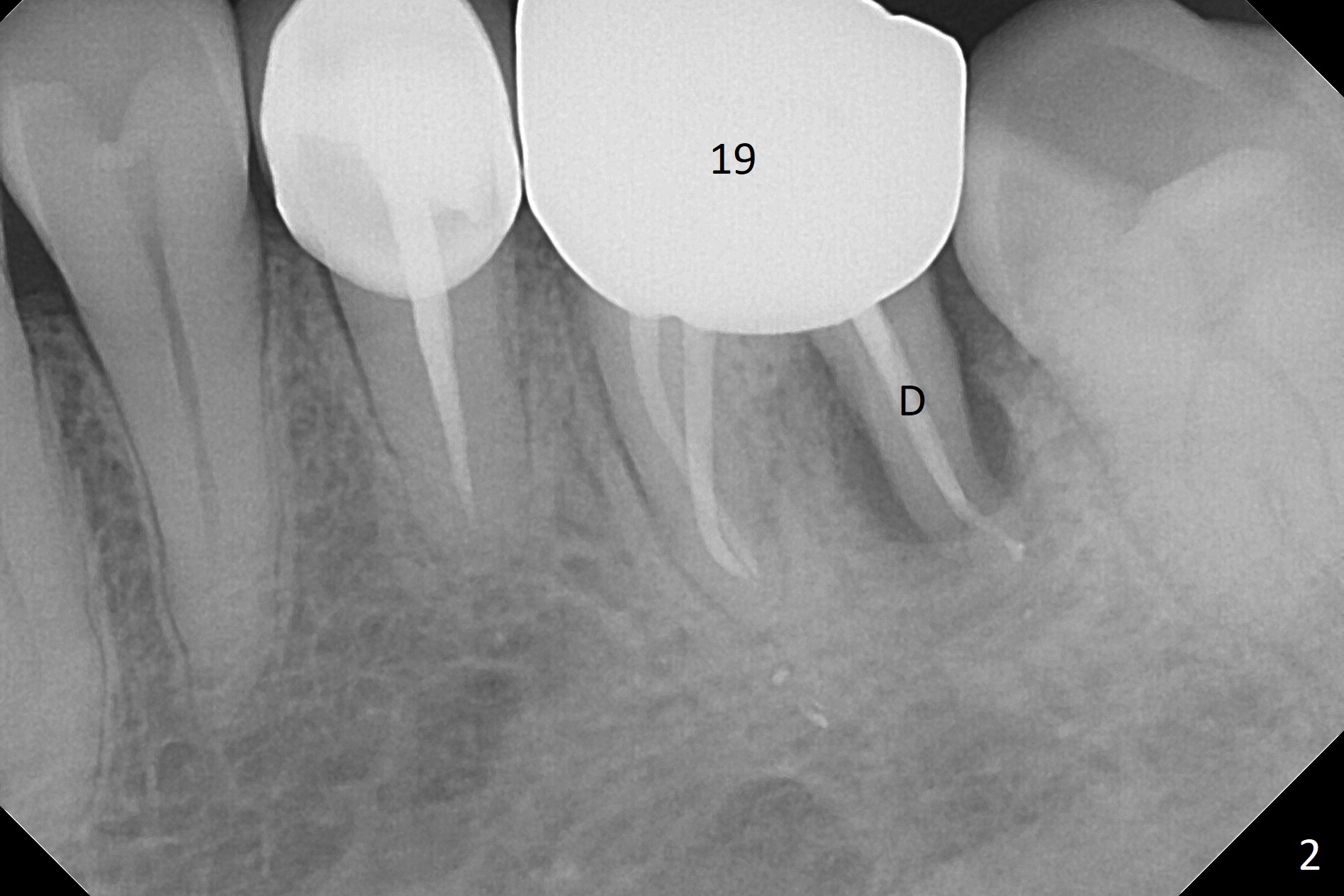
Distal Root Fracture
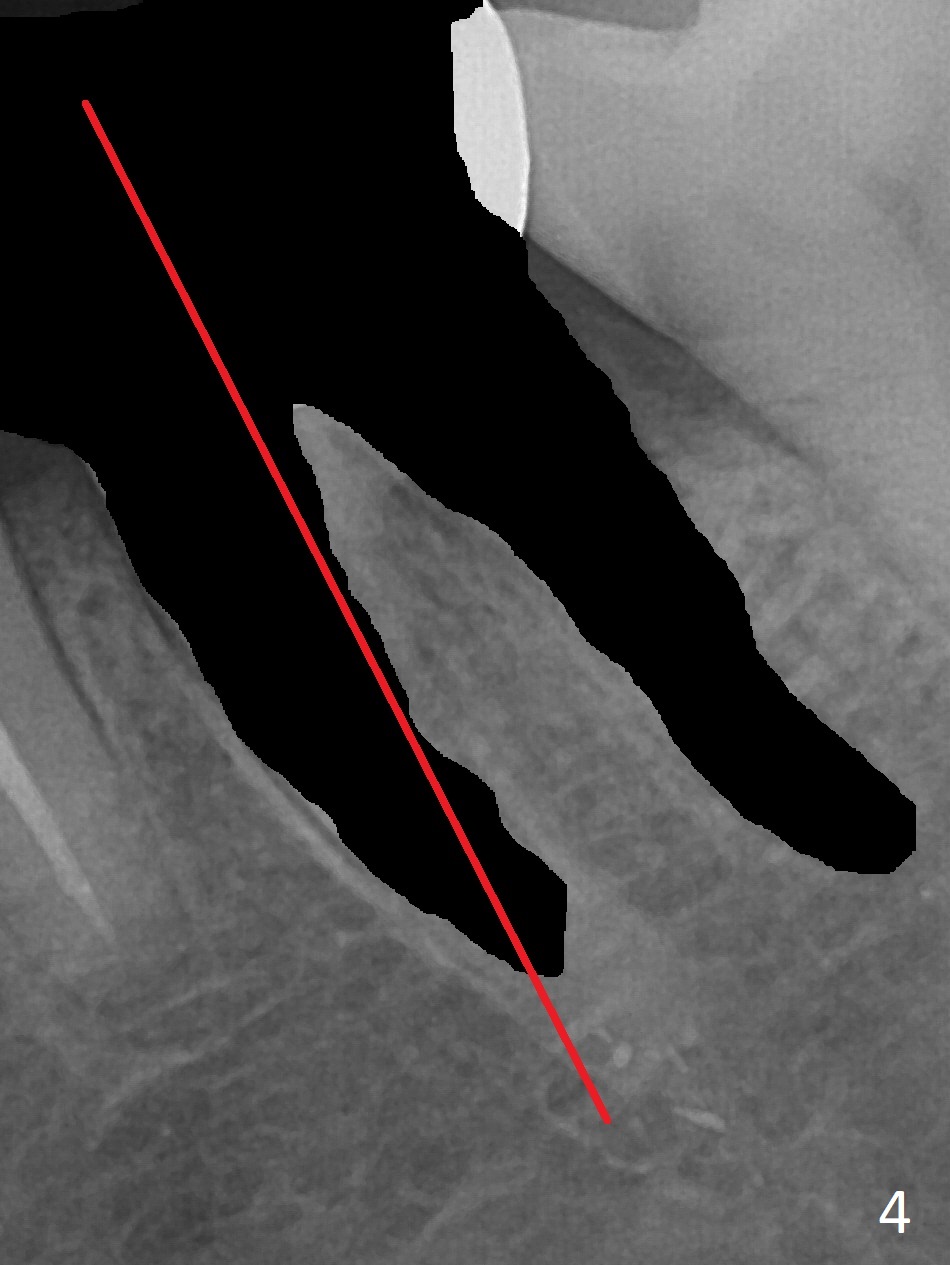
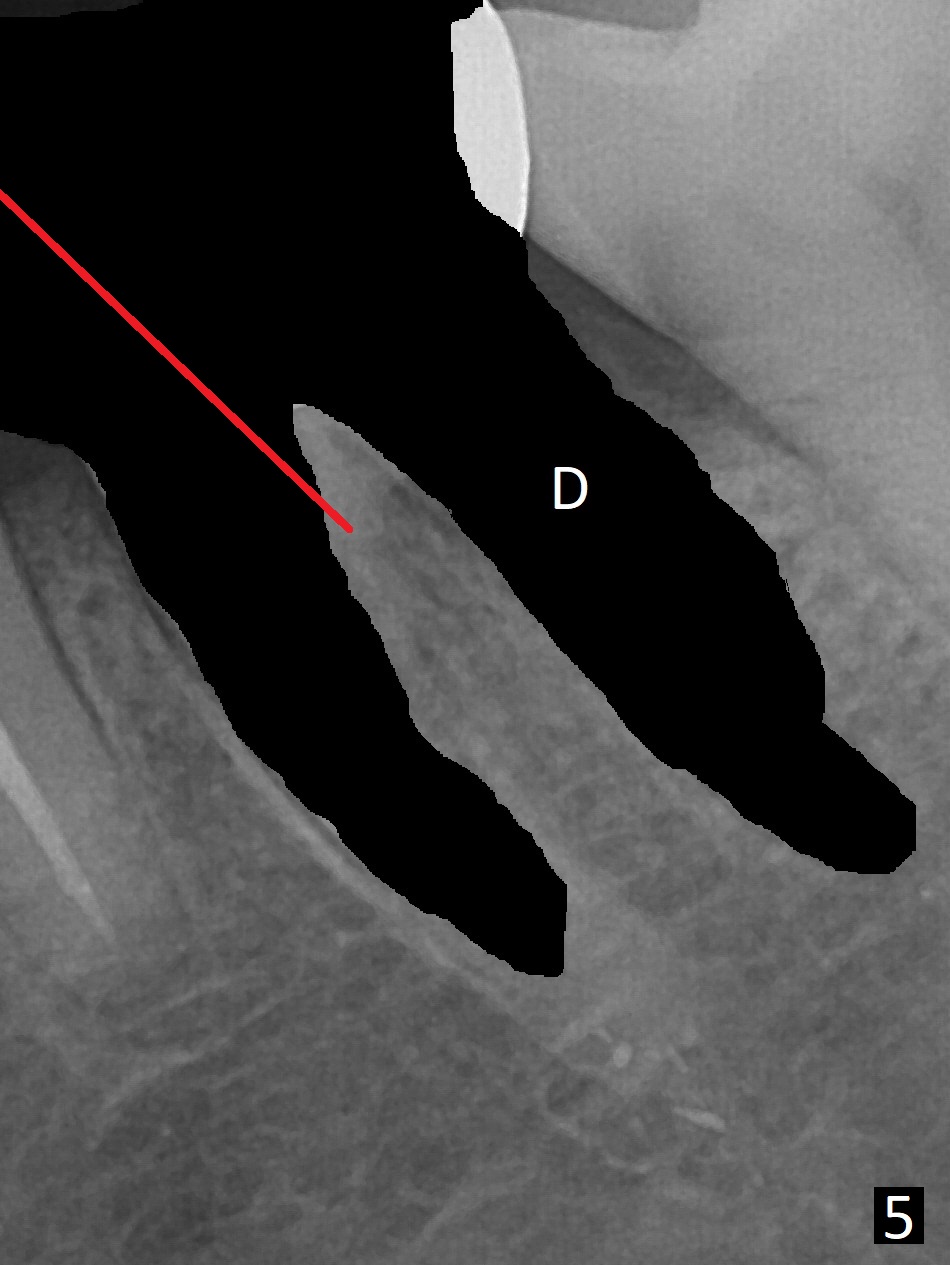
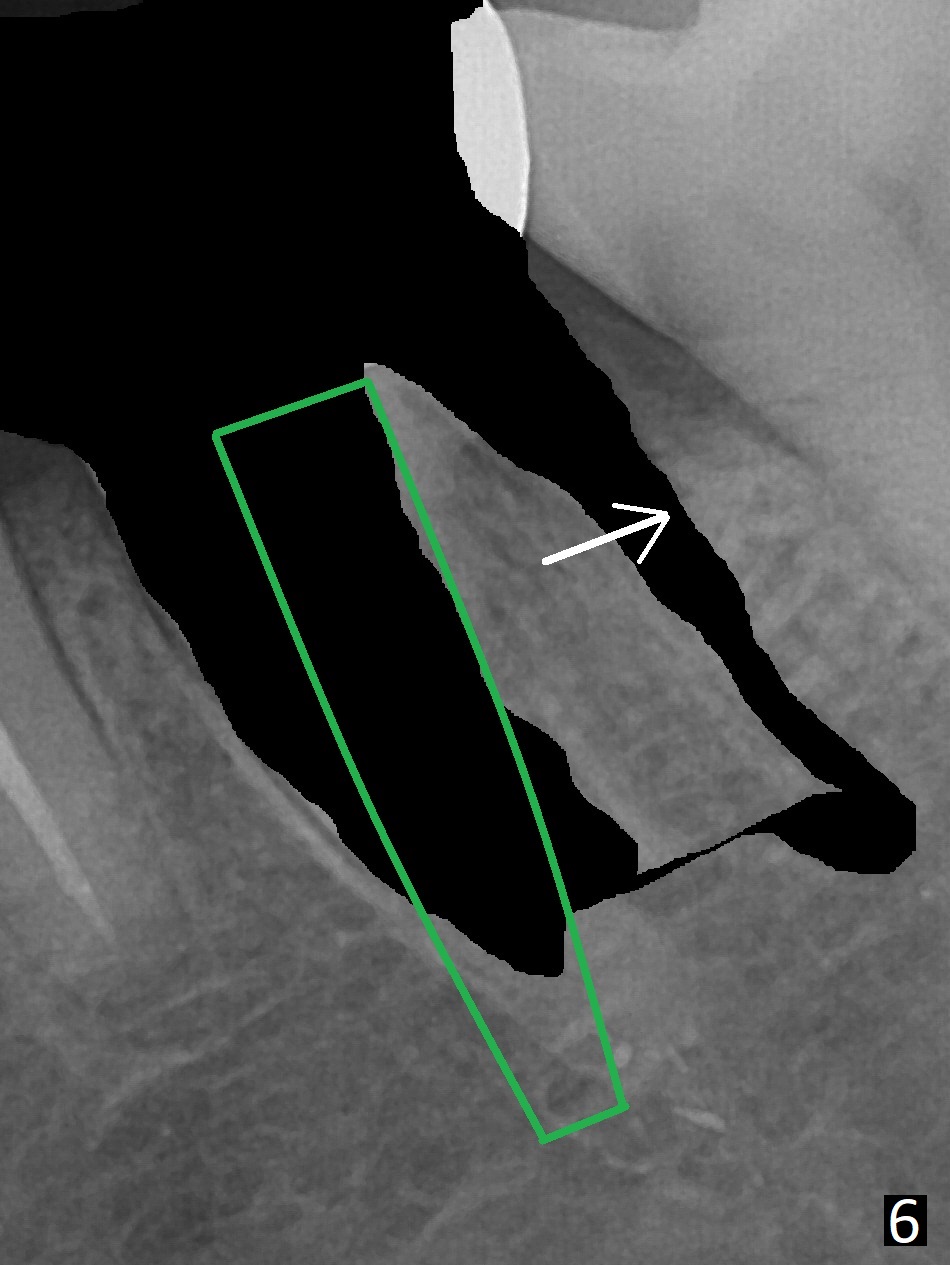
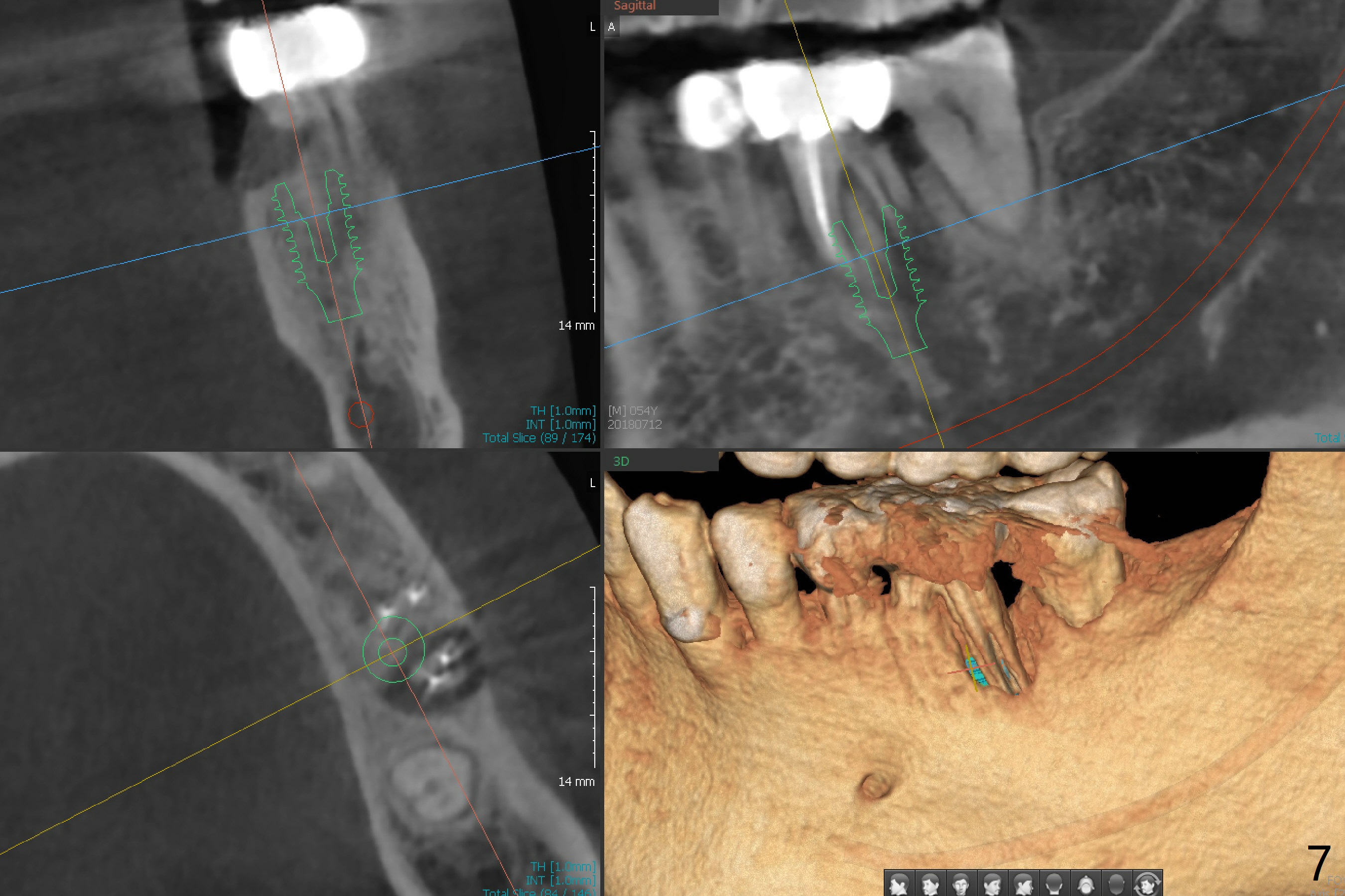
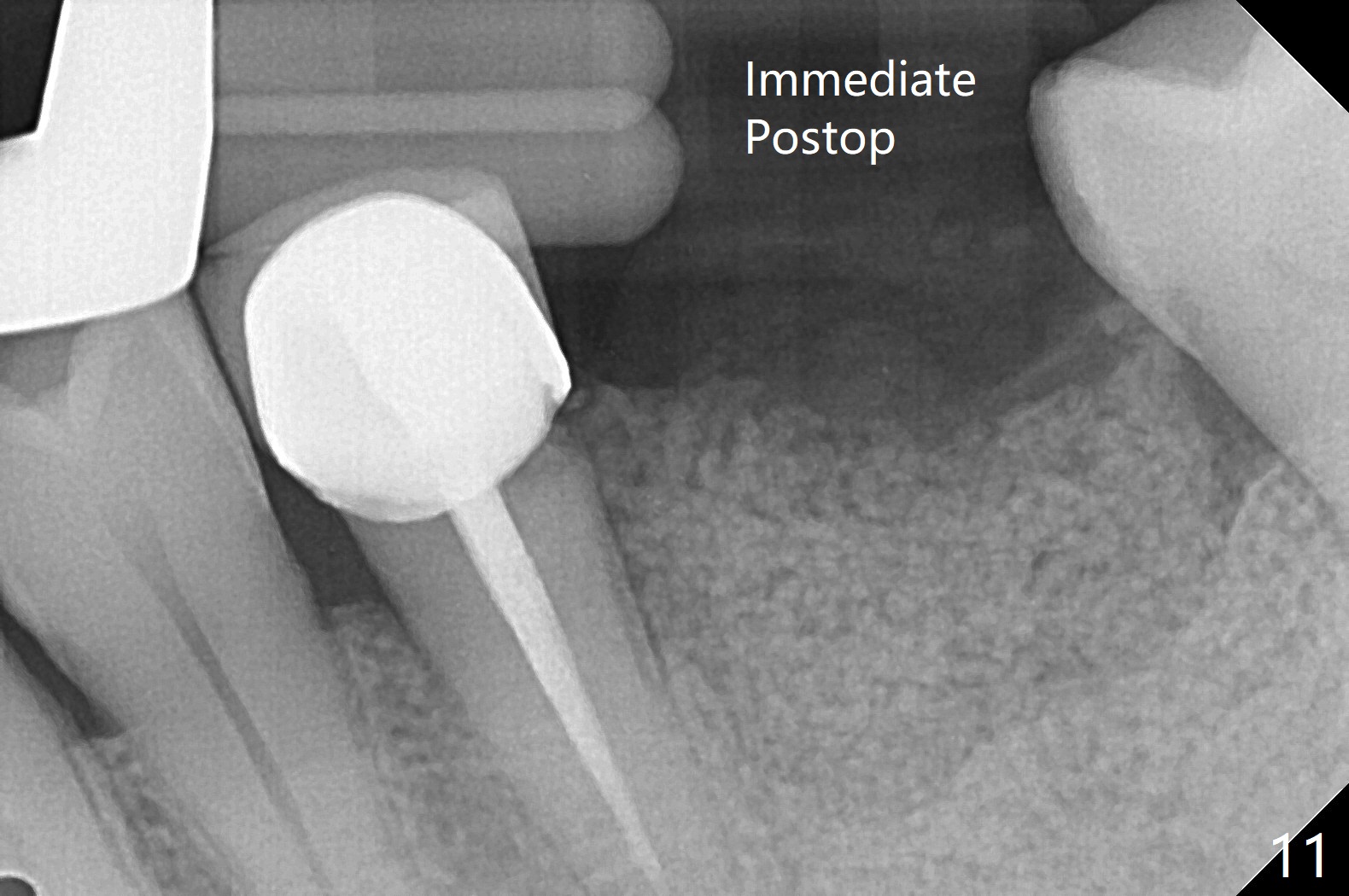
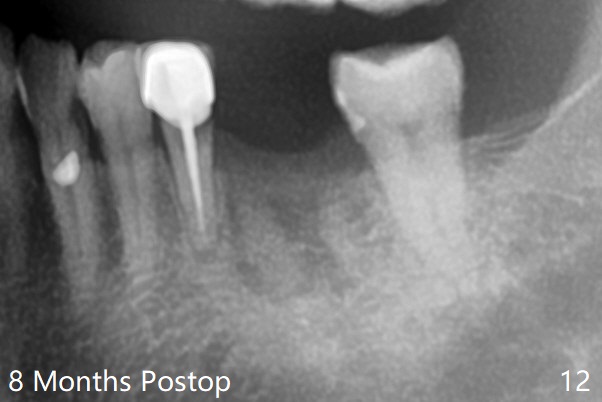
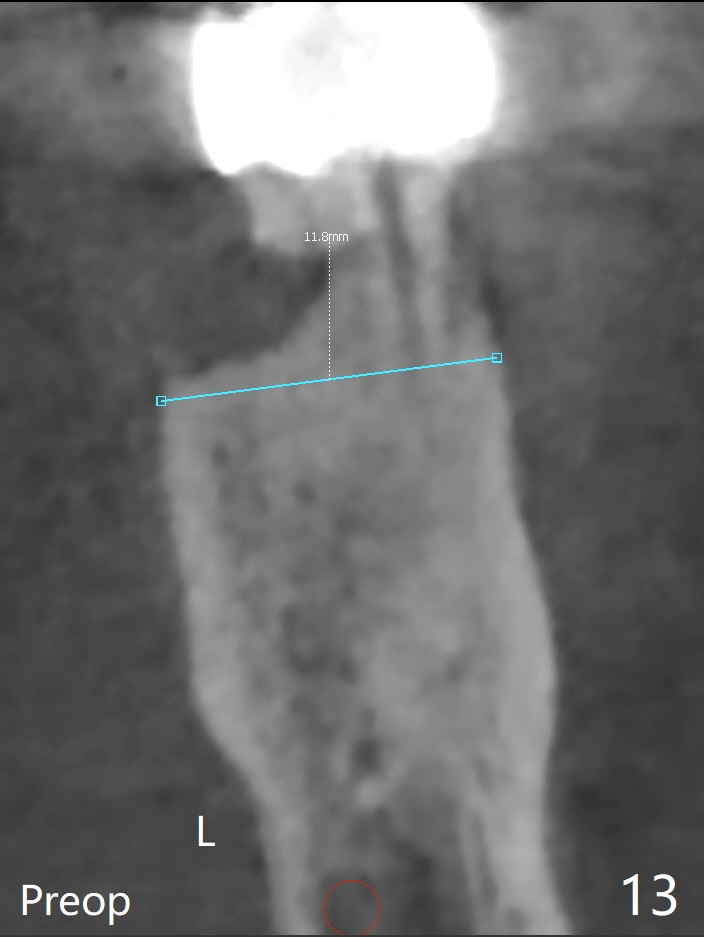
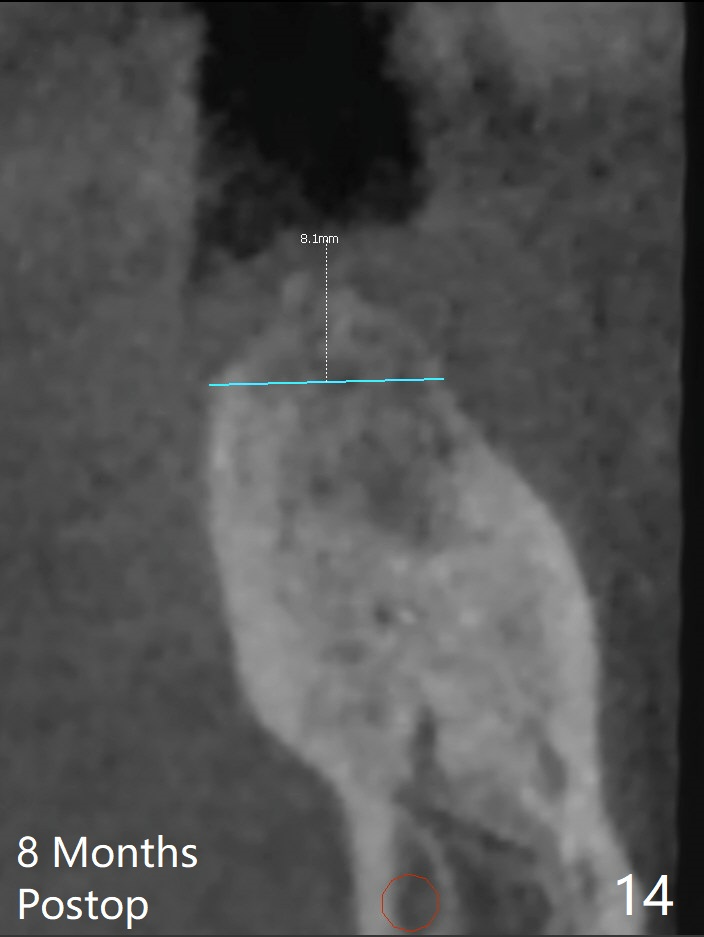
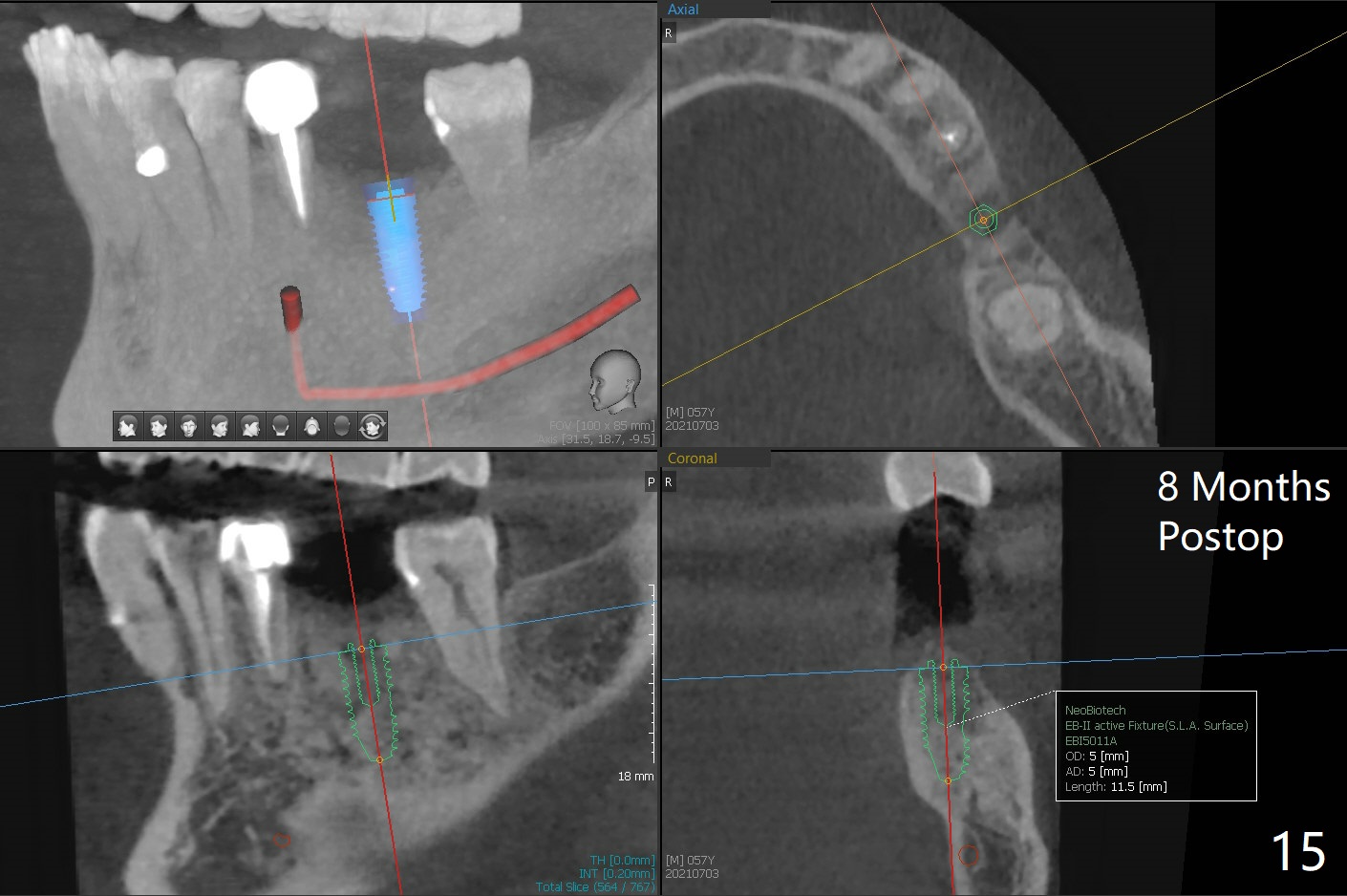
A 54-year-old man has distal (D) root fracture at #19 while the implant at #2 is osteointegrarting (Fig.1,2). Because of the large distal defect (Fig.3, after extraction), osteotomy (red line) will be initiated in the mesial socket (Fig.4, as distal as possible, with the coronal end in the middle of the socket) or the mesial slope of the septum (Fig.5) so that the implant (green) will be supported by the distally displaced septum (Fig.6 arrow). CT taken 8 months later confirms distal root fracture. A 6x11.5 mm or longer implant seems to be appropriate for the site (Fig.7). Three years later there is severe buccal swelling (Fig.8) with vertical mesial and distal root fractures (Fig.9). Although the buccal plate is lost, the septum remains (Fig.10 S), which will provide with blood supply to the bone graft (Fig.11), covered with Bioxclude and 6-month membrane and PSA suture. The bone density in the mesial and distal sockets is higher than that in the septum 8 months post cortical bone graft (Fig.12). In spite of bone graft, the buccolingual width reduces by almost 4 mm 8 months post extraction (Fig.3,4). In spite of bone graft, the buccolingual width reduces by almost 4 mm in 8 months post extraction (Fig.3,4). A 5x11.5 mm implant will be placed (Fig.15).
Return to
Lower
Molar Immediate Implant, Prevent
Molar Periimplantitis (Protocols,
Table),
IBS,
Armaments,
No Antibiotic,
No
Caries
#7,10
3
位点保存
Xin Wei, DDS, PhD, MS 1st edition 11/26/2017, last revision 07/04/2021