


|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
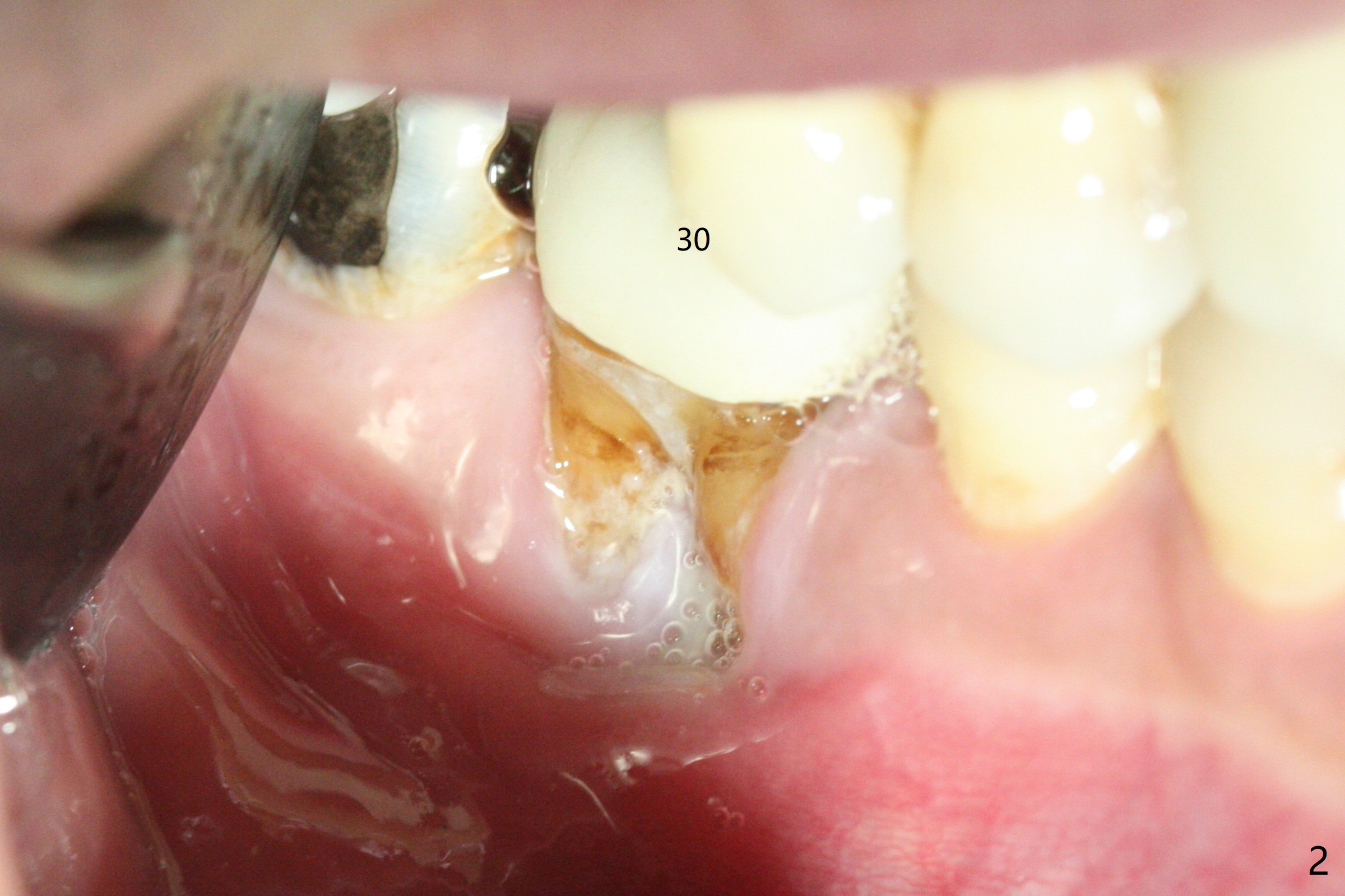
Buccal Root Exposure
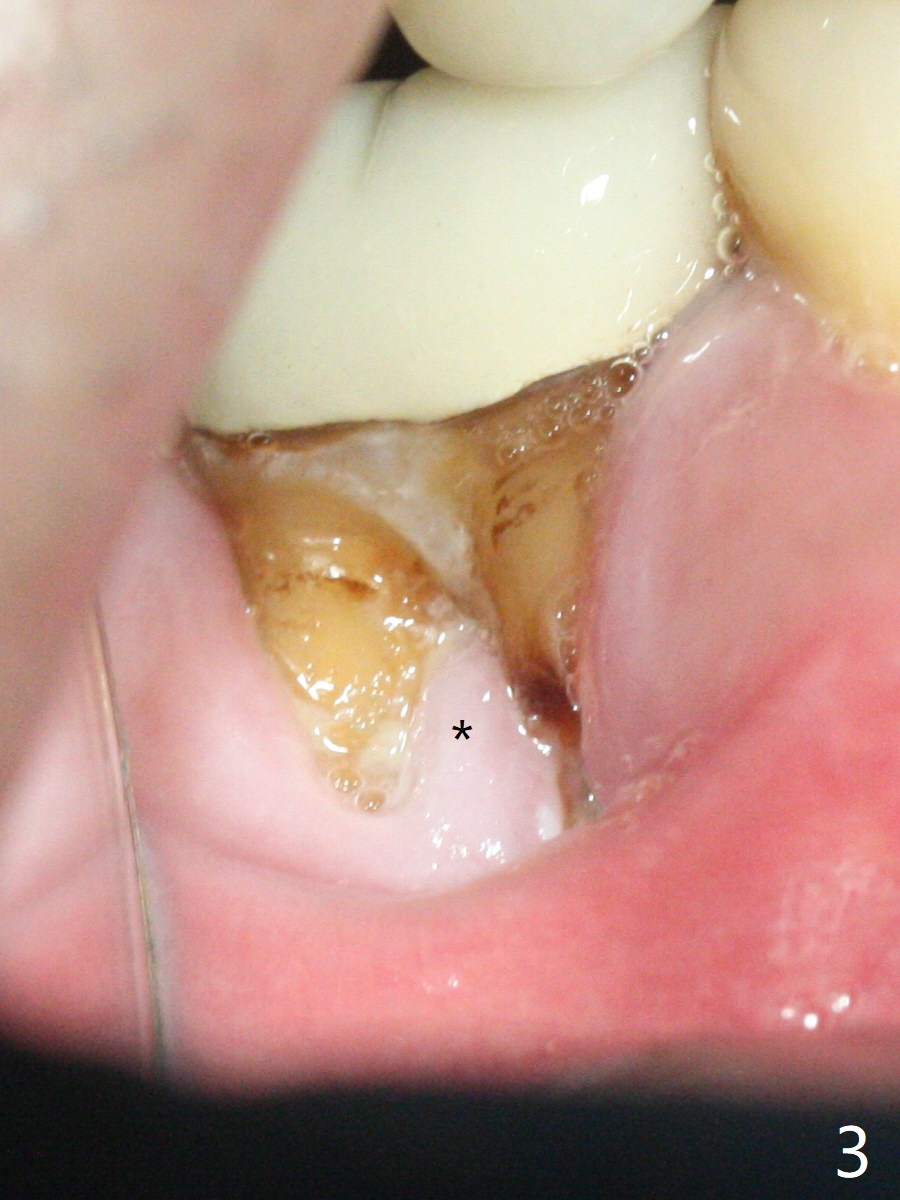
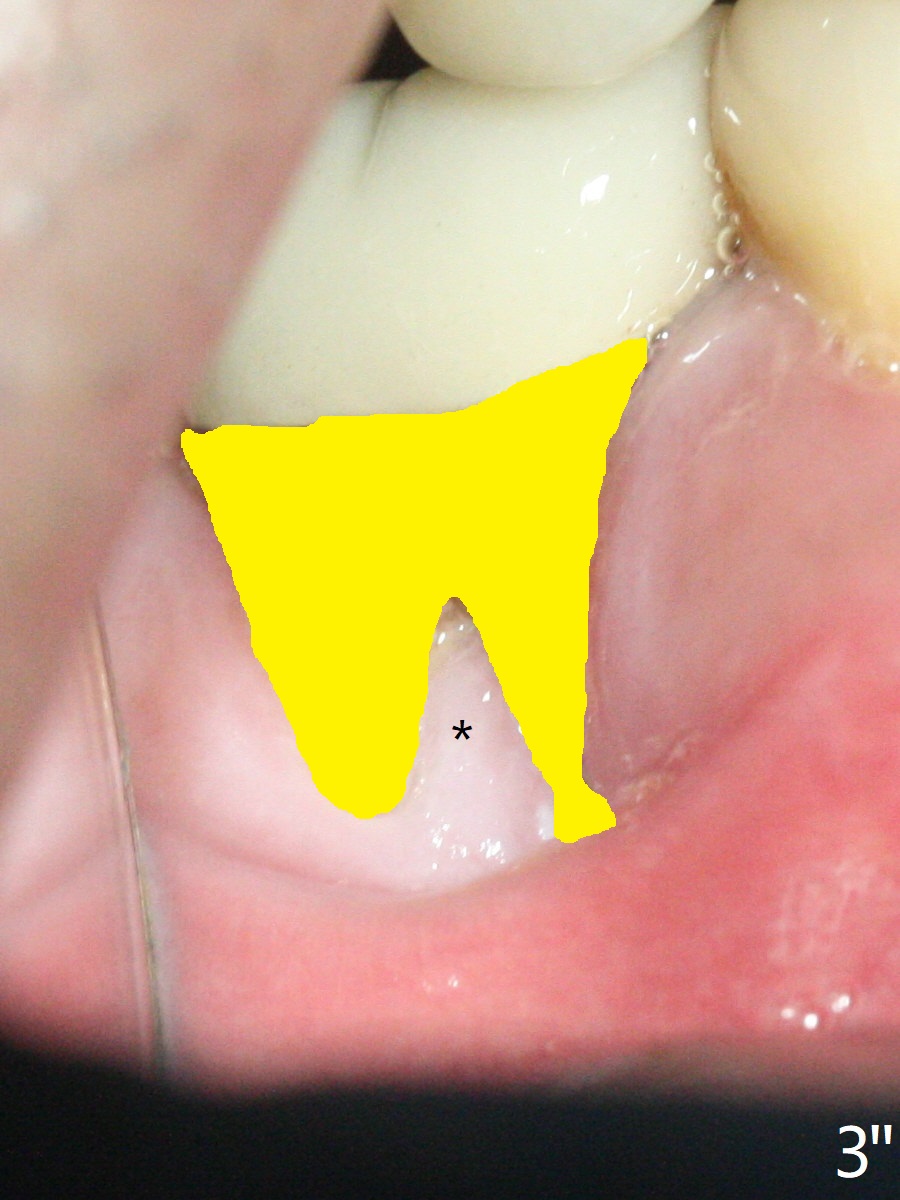
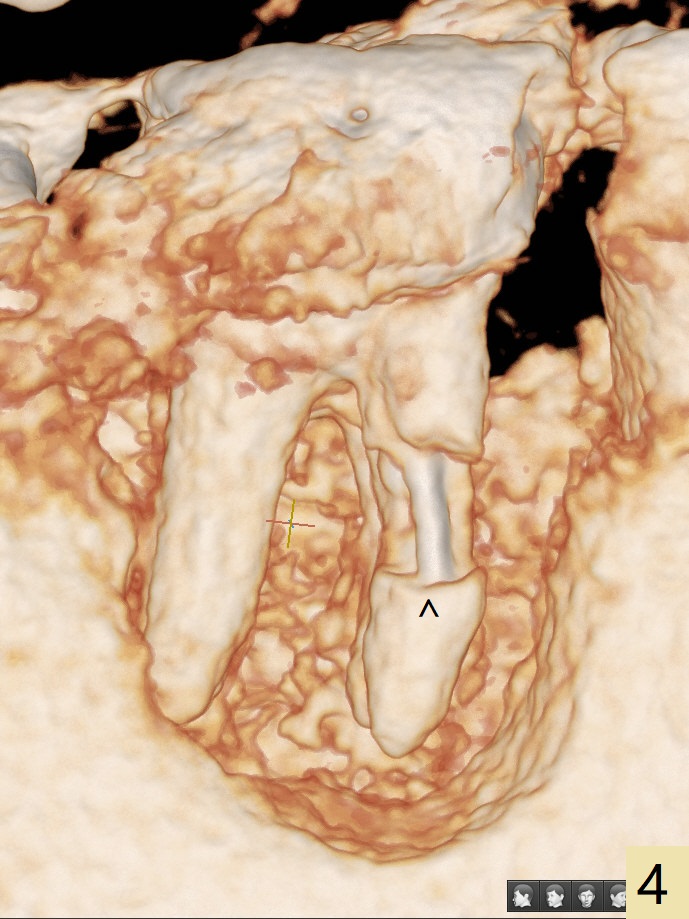
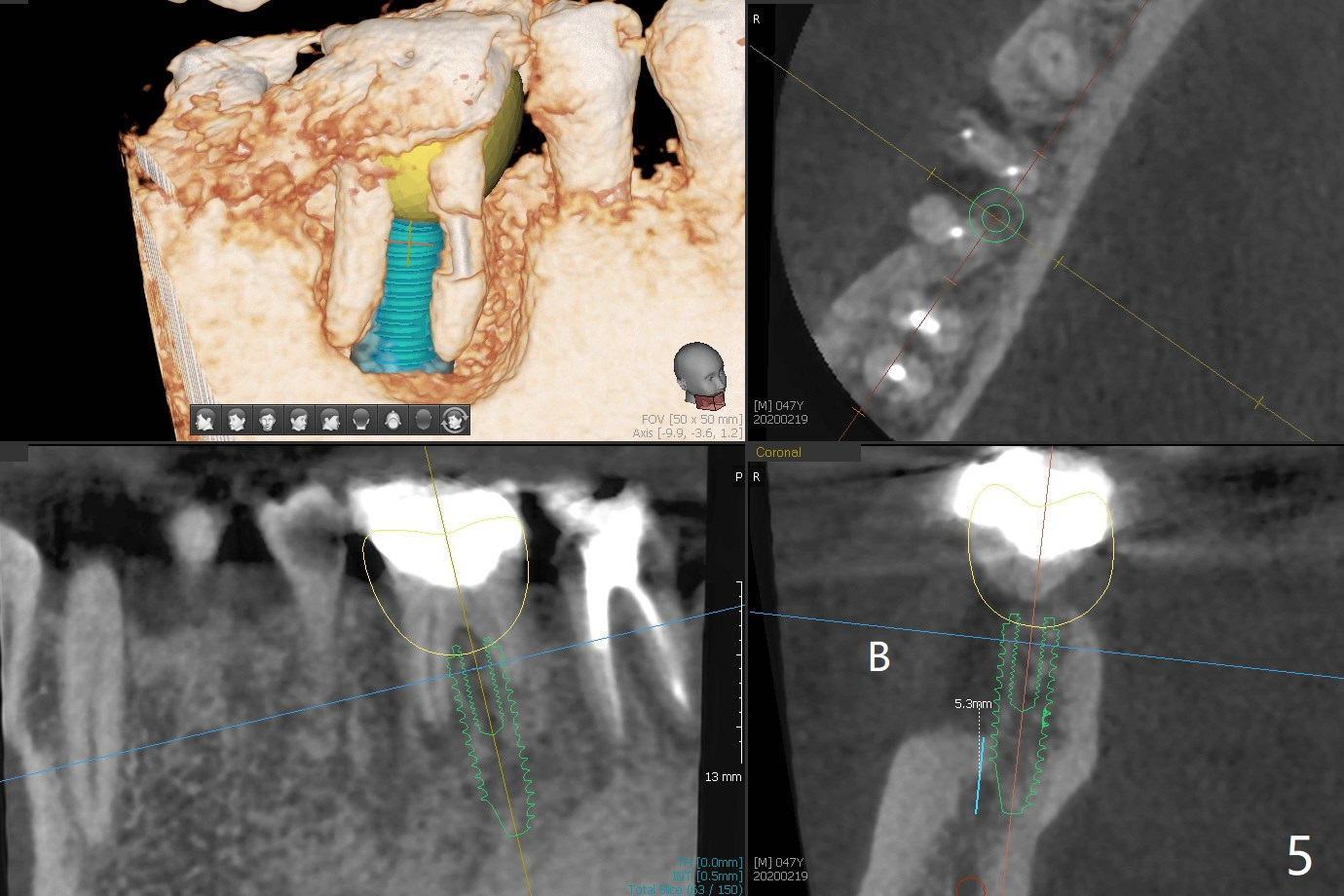
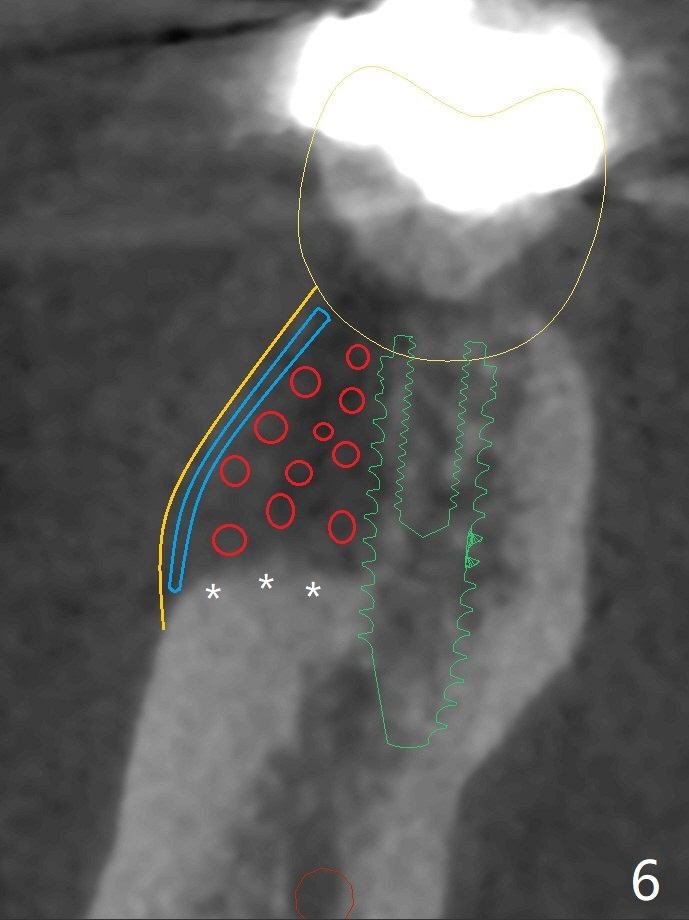
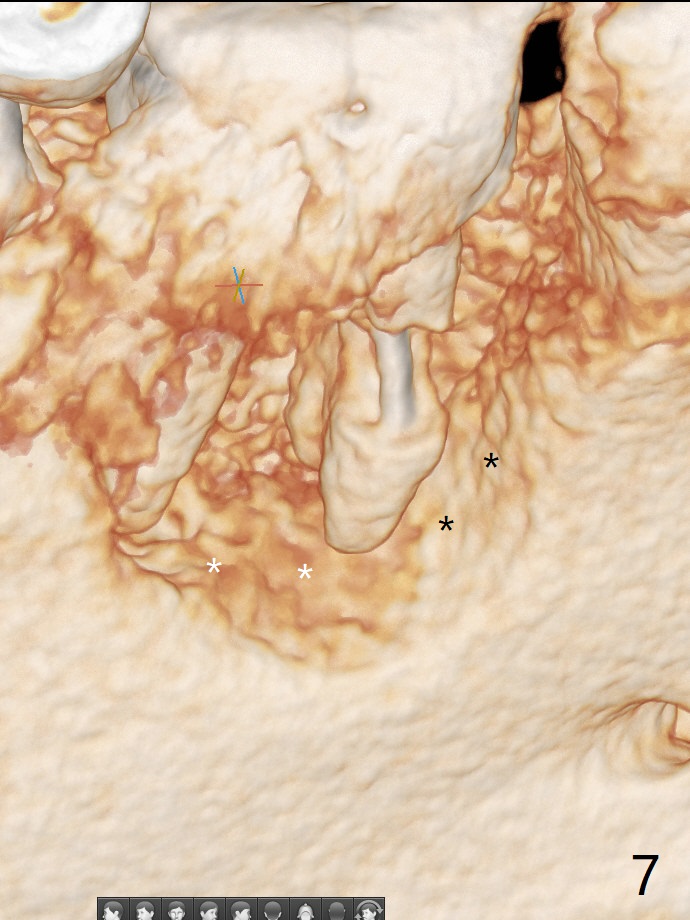
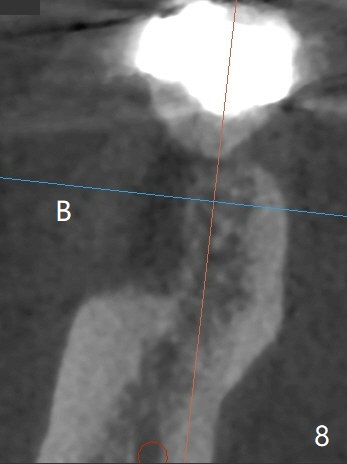
A 47-year-old man has poor dentition. The tooth #31 needs RCT, while #30 has severe PARL, especially mesial (Fig.1 M). The buccal roots are exposed (Fig.2). Between the exposed roots is the septal gingiva, which will be saved for buccal soft tissue repair (Fig.3 *). The septal gingiva will keep in place (not to be transferred) so that the recession will disappear by epithelial regrowth from the nearby gingiva (Fig.3' arrows) over the bone graft and PRF. The provisional should be fabricated to cover the soft tissue defect (Fig.3'' yellow area). In fact the mesial root fractures (Fig.4 ^), as related to the severe bony defect. There seems to be enough lingual bone to hold a 4x13 mm implant (Fig.5 green). Sticky bone (Fig.6 red circles) and PRF (blue) are to be used to repair the hard and soft tissue defects following an immediate provisional (Fig.5,6 yellow outline). Extra layer of acrylic (Fig.6 orange) will be used to cover the PRF buccally. The base of the buccal plate is thick (Fig.6 *); mesial portion appears to be denser (Fig.7 black *) than the distal one (white *). Decortication will be done if hemorrhage is insufficient. Fig.8 is a coronal section of the socket (B: buccal). Extraction (Fig.9 black area) will most likely result in a knife edge ridge. Extraction with bone graft may not fare better, as it is easy to lose the graft considering missing buccal hard and soft tissues.
Return to
Prevent Molar Periimplantitis (Protocols,
Table)
No Deviation
No Antibiotic
6 Proximal
Sheath
Xin Wei, DDS, PhD, MS 1st edition
02/16/2020, last revision
05/13/2020