

.jpg)





|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Soft Bone of Smoker
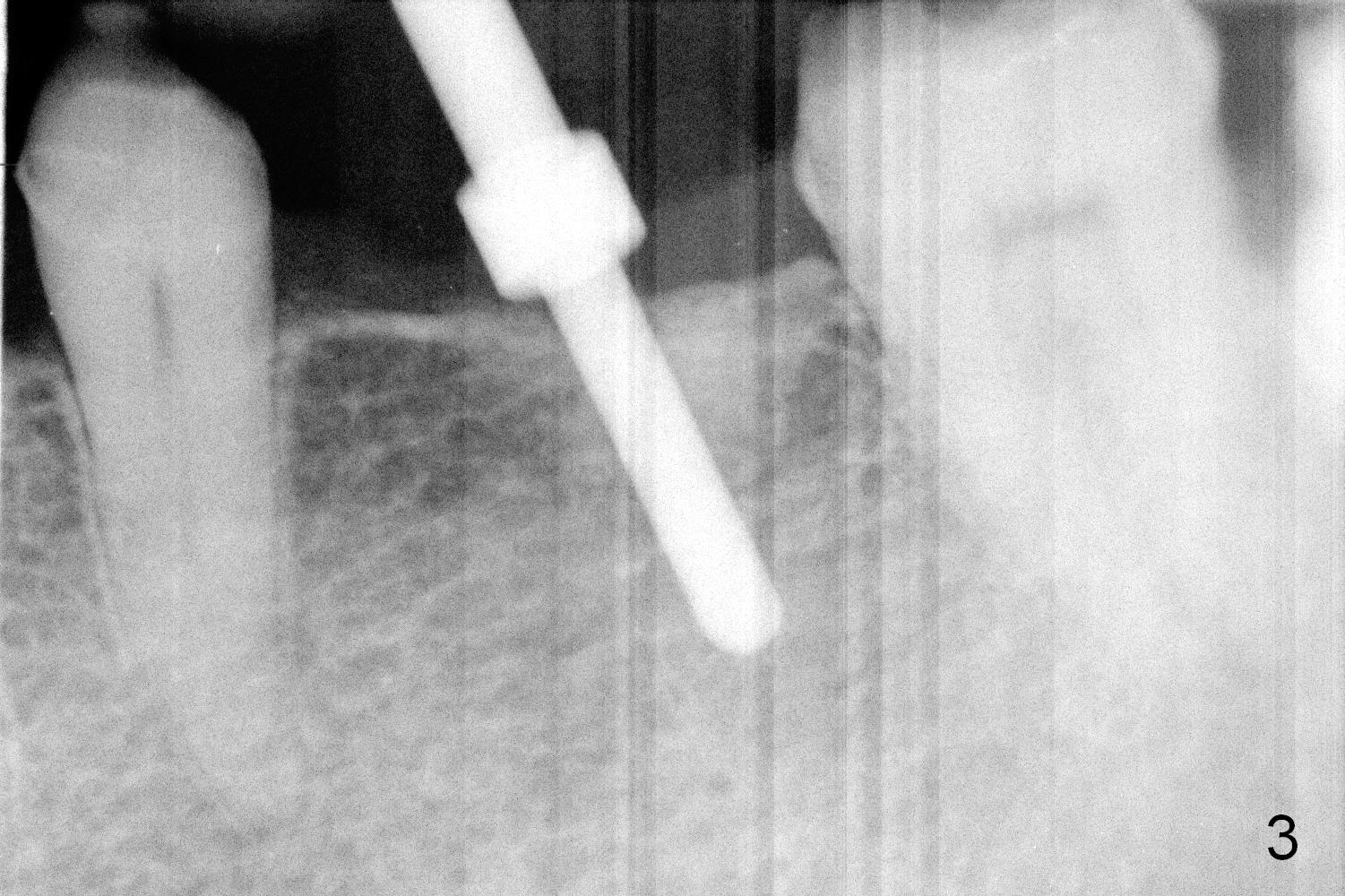
When the patient returns for implant placement, he is pleased to let us know that he has stopped smoking for a week. The edentulous ridge at #19 looks wide (Fig.1). The tooth #3 is supraerupted, while there is no clearance between the abutments (#18 and 20) and the opposing dentition (Fig.2). After incision, the ridge is confirmed to be wide with the aid of implant positioners. The bone is felt soft during initial osteotomy (Fig.3). Attention is being paid to correcting the trajectory. Under prep is ignored. When a 5.9x10 mm implant is placed, the insertion torque is between 25 and 30 Ncm (Fig.4).
Since the implant is placed subcrestal mesially (Fig.4 >), the mesial margin of the abutment (5.8x4(3) mm) is subgingival (Fig.5 ^). An immediate provisional has to be made to keep the gingiva from growing into the margin. After occlusal clearance (Fig.6), the immediate provisional is seated (Fig.7). There is no paresthesia postop.
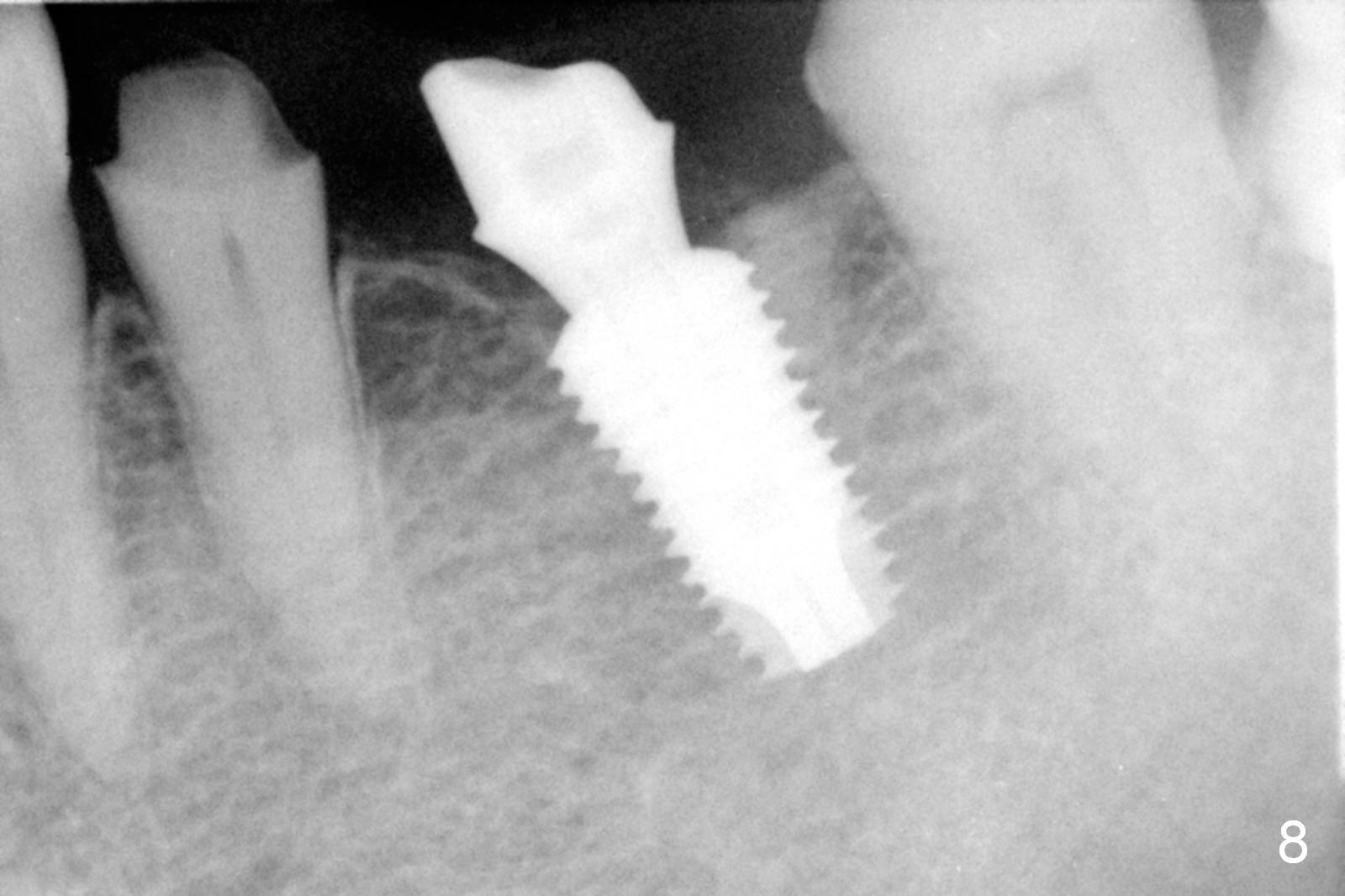
The patient returns for restoration 13 months postop with implant osteointegration (Fig.8) and formation of gingival cuff around the implant/abutment (Fig.9 *). In fact the immediate provisional seems to help mastication to certain degree (Fig.10). Probably it has resisted supraeruption of the opposing dentition. Impression is taken without torque of abutment screw. He smokes again.
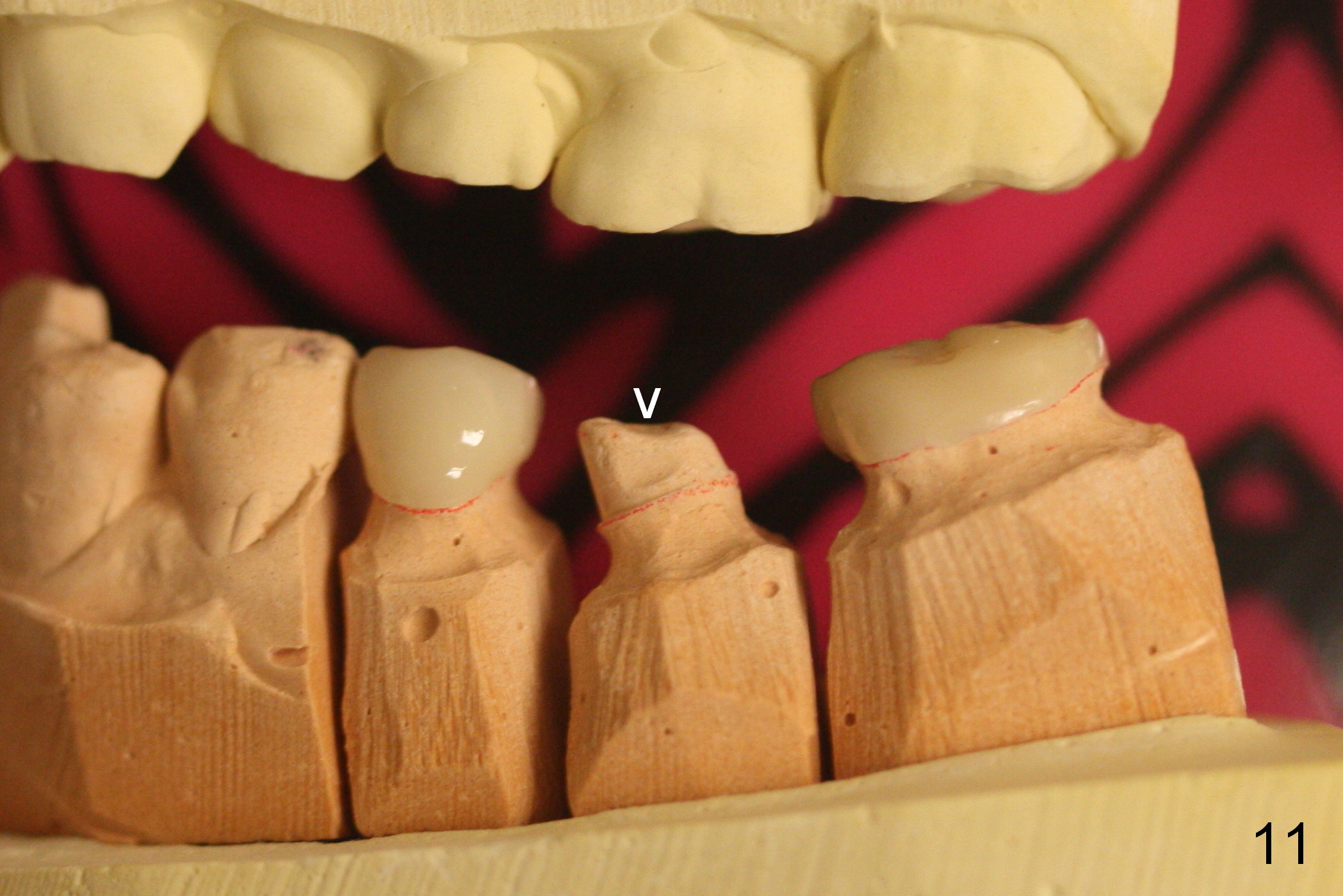
The access is mesial at #19 (Fig.11 v). After cementation, the abutment screw is torqued through the access, which is then closed with flowable composite (Fig.12 *).
Return to
Lower Molar Immediate Implant,
Systemic Disease,
Posterior Immediate Provisional
Xin Wei, DDS, PhD, MS 1st edition 07/12/2015, last revision 08/29/2016