










|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
Atypical Extraction
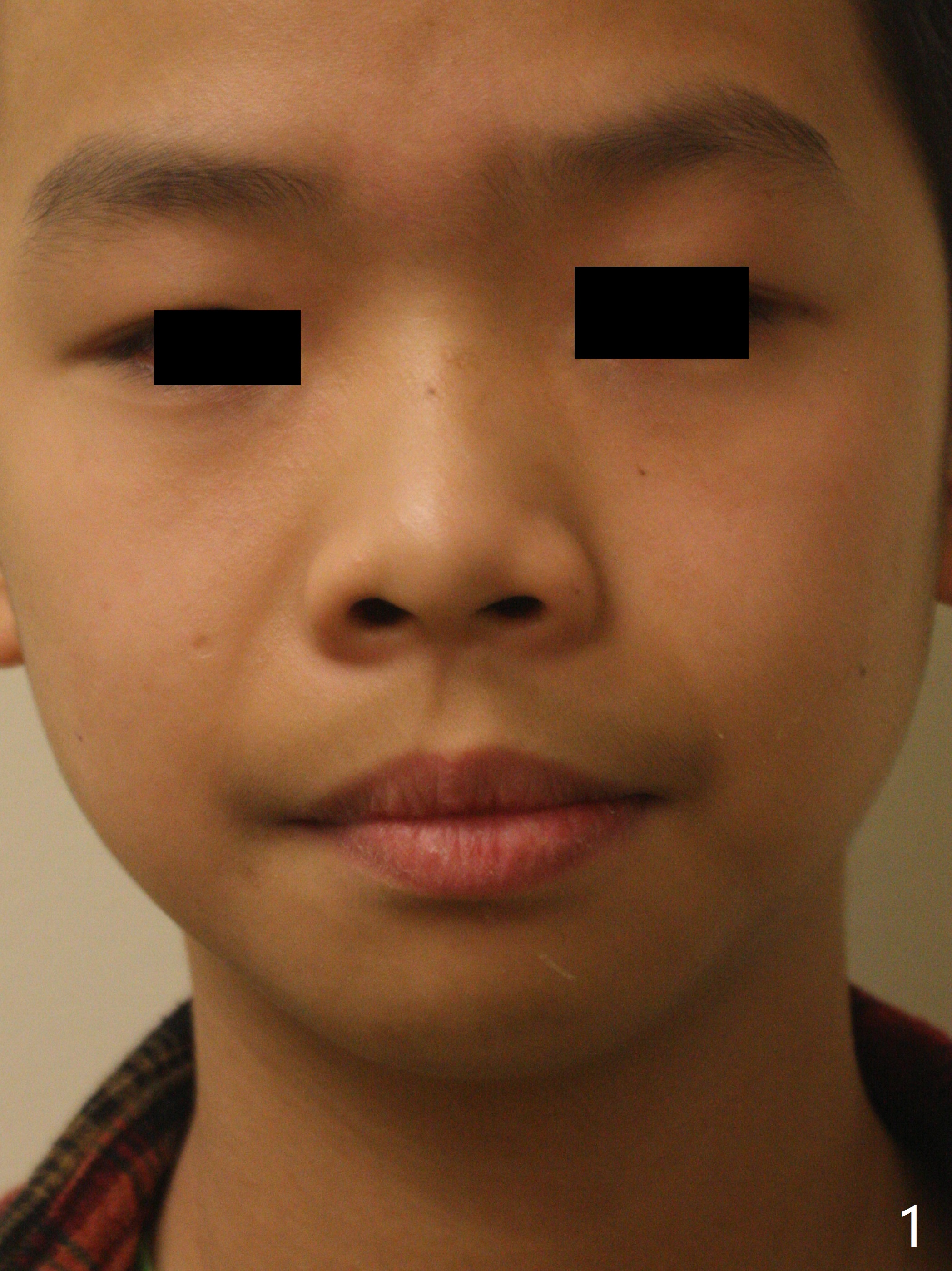
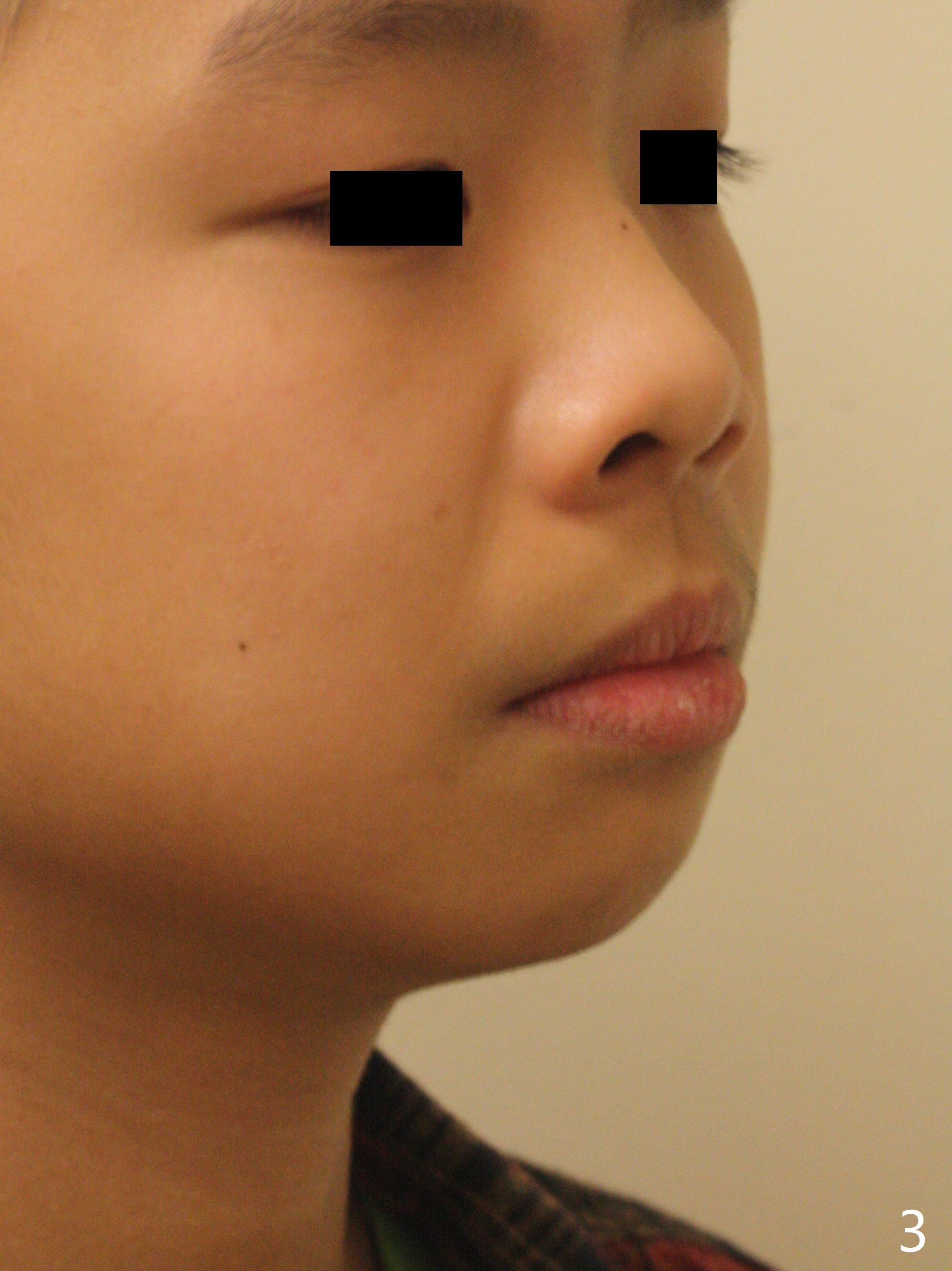
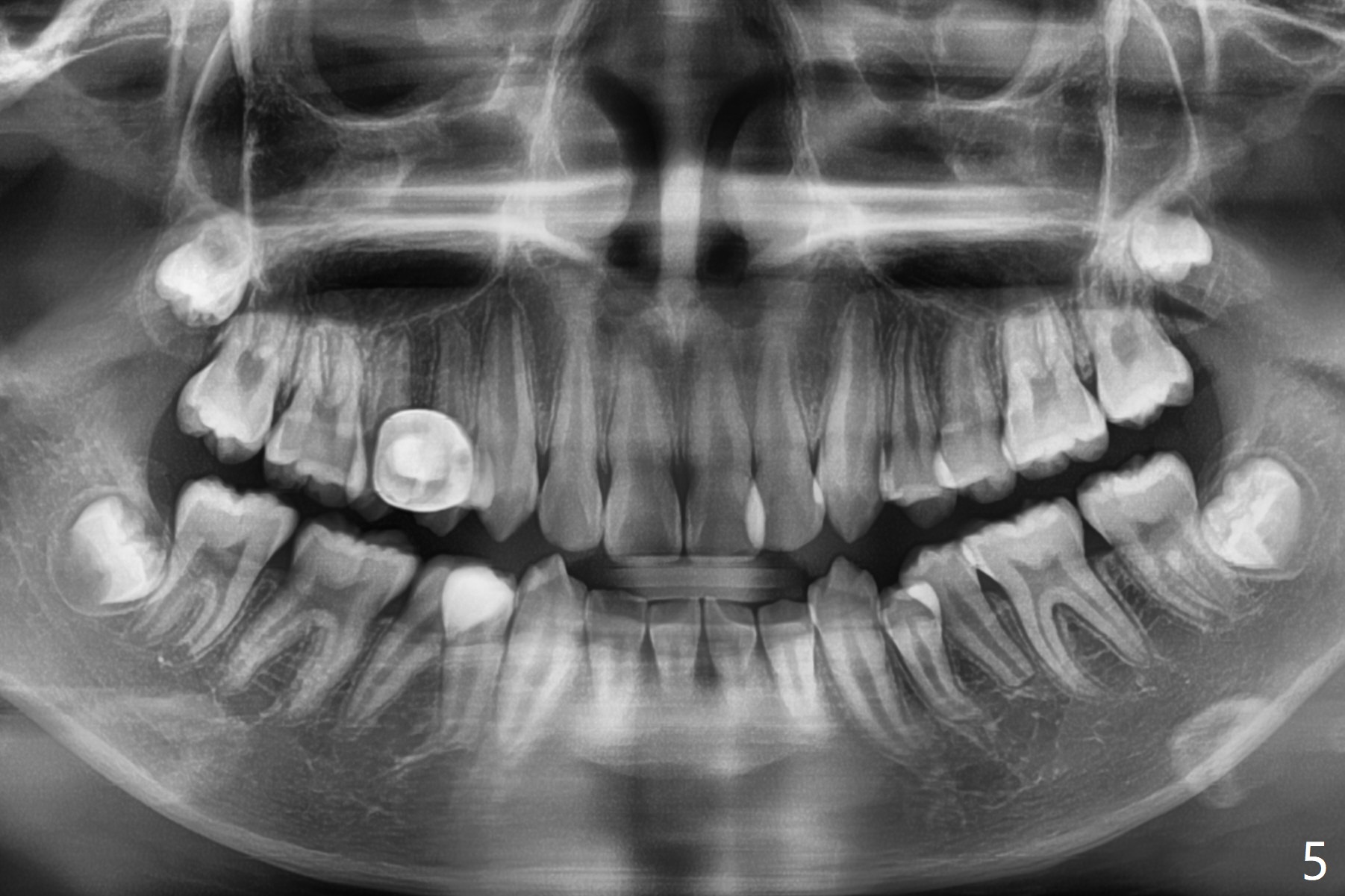
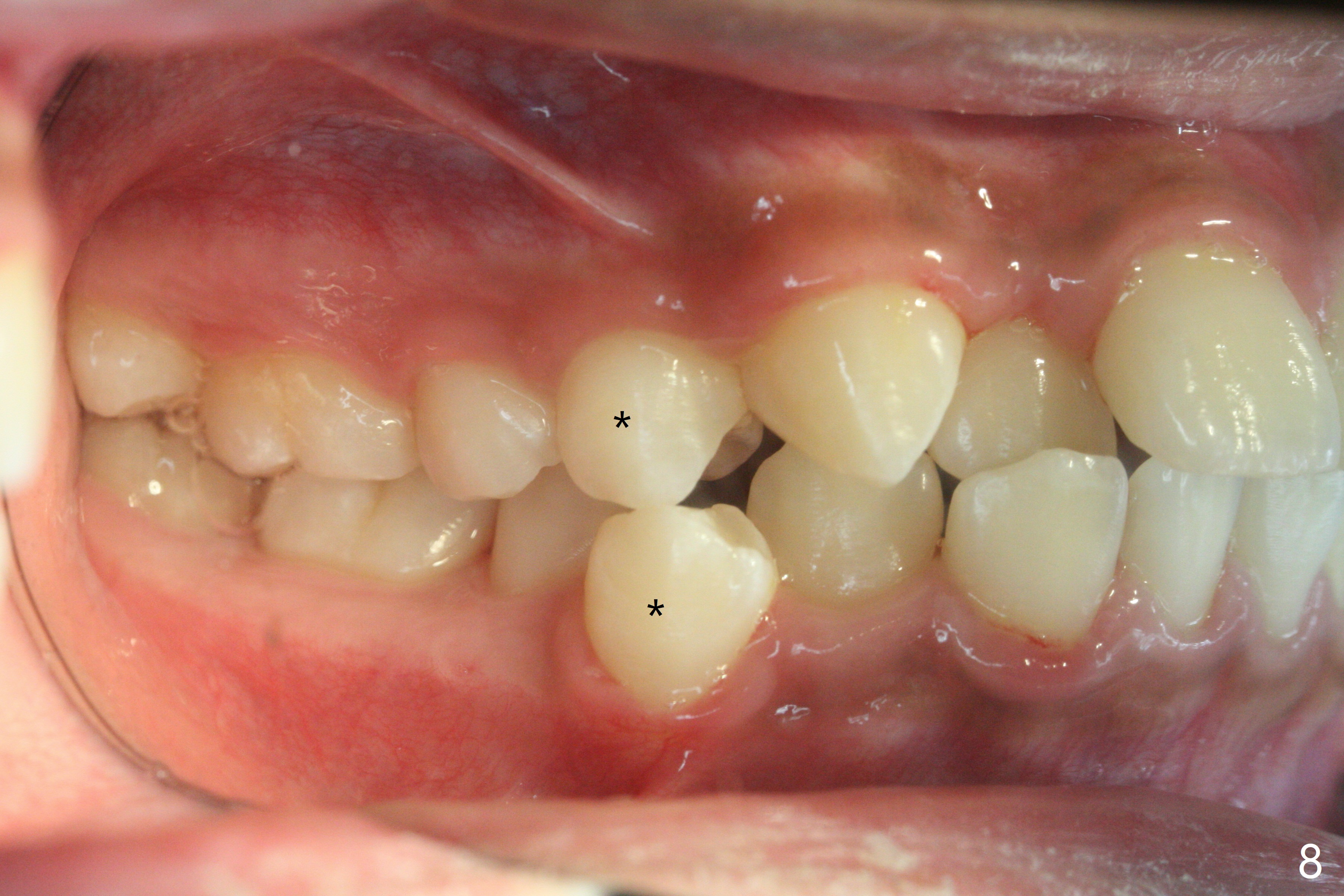
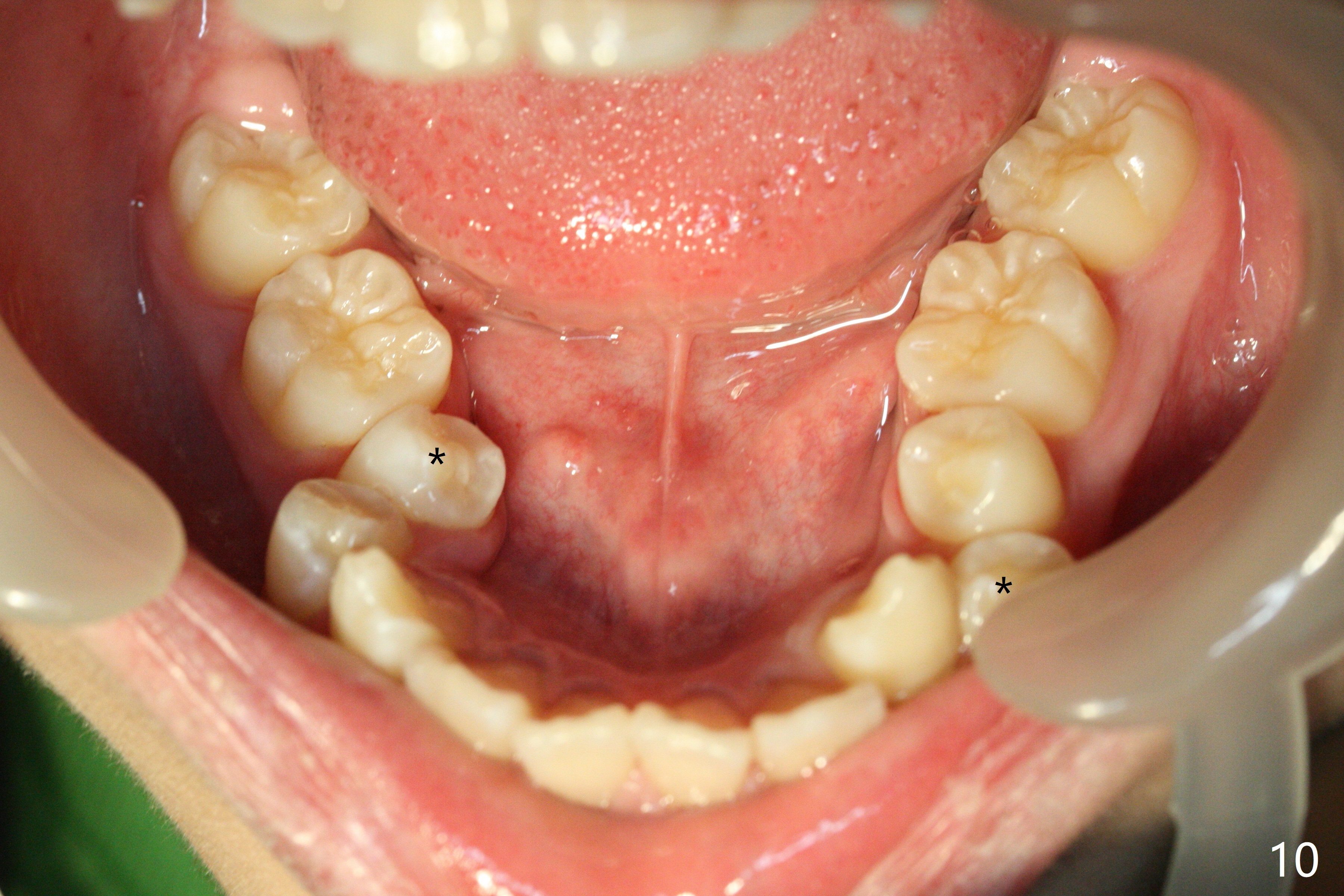
A 13-year-old man has protrusive lips (Fig.1,3,4) with upper midline deviation to the left (Fig.2). Crowding is severe with LR5 severe lingual inclination (Fig.5,6,10). To facilitate L6s' uprighting (Fig.10), LR5 and 3 of the 1st bicuspids will be extracted (Fig.6-8 x or *) and molar bands with lingual cleats will be used for the lower. Cross arch molar retraction will be initiated immediately. Open coil spring will be placed between UL1 and 3 with the 1st wires to correct the upper midline deviation and to gain the space for UL2.
The patient will return 2 months post extraction. Shifting is expected to occur next to extraction sites (*) as indicated by arrows in Fig.9,11. Take photos if it is the case. Place bracket at UL2 if there is no space issue, but upside down (why?). The most flexible wire is anticipated. To establish Class I occlusion when wires are stiffer (18ss), LL5,6 will be mesialized as equally as LL3 distalized, while UL5,6 maintained basically in situ (Fig.11). How to accomplish?
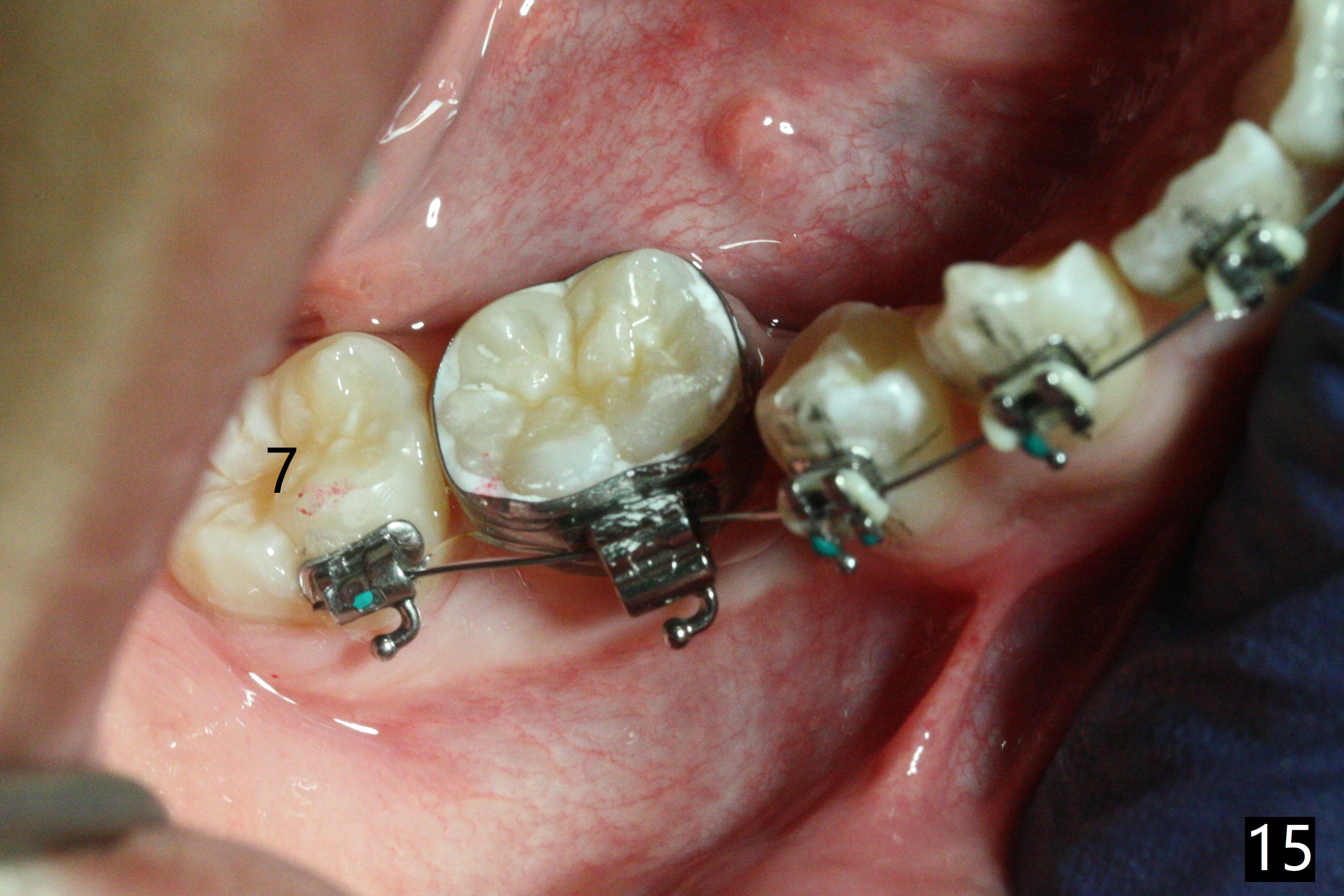
In fact, automatic shifting is striking. For example, UR5 lingualization (Fig.12 arrow) makes it easy to insert 12 niti wire. Distalization of the lower bicuspids and canine is more obvious (Fig.13,14 arrows) than the upper counterparts. Because of incomplete eruption, it is difficult to band L7s; instead brackets are placed (Fig.15-17). The purpose of LR one is to facilitate LR6 buccalization (Fig.15,16), whereas LL one to correct rotation of itself (Fig.17).
Xin Wei, DDS, PhD, MS 1st edition 02/04/2018, last revision 10/04/2020