



|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|||
Where to Graft Around Immediate Implant
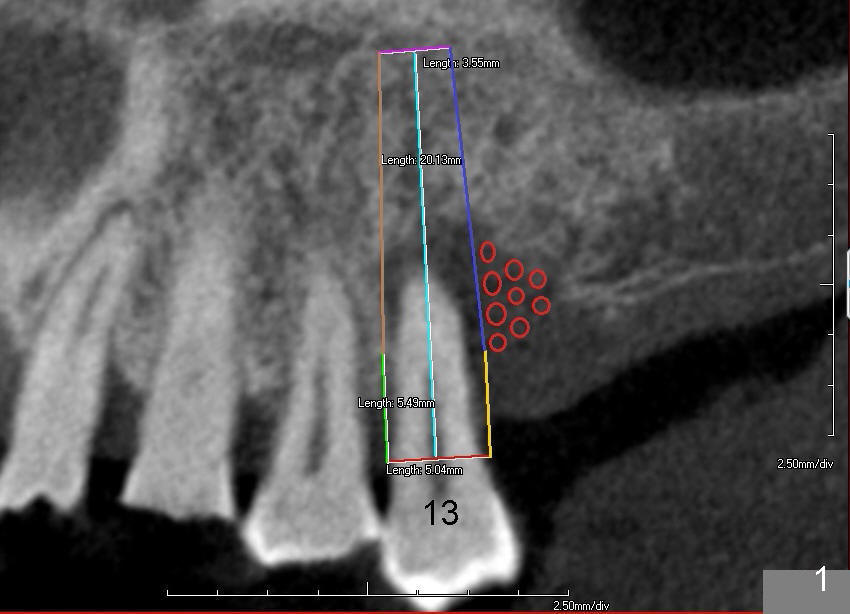
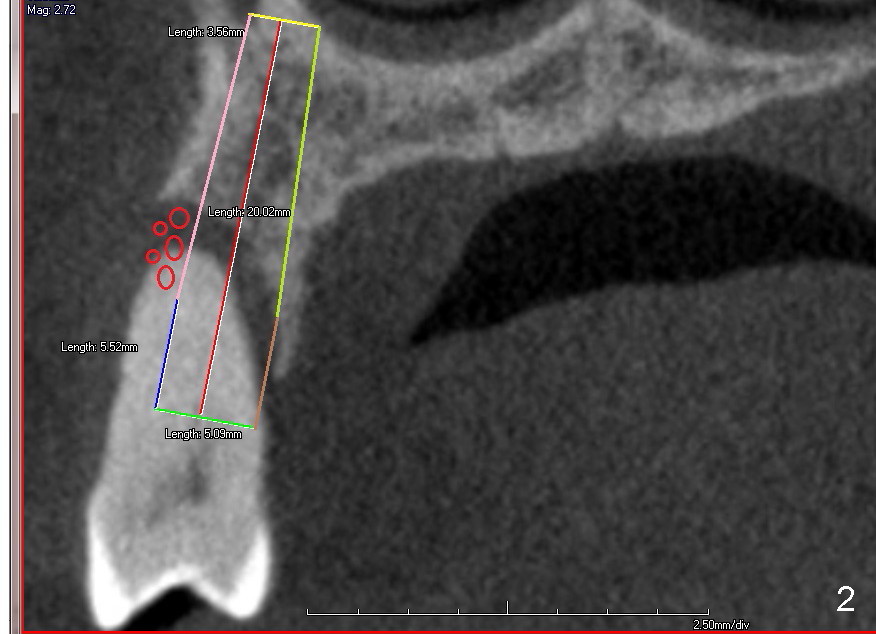
Immediate implant at the site of #13 is the last implant to be placed for full mouth reconstruction (Fig.1 CT sagittal section; 1 2 3 4 5 6 7 8). The sequence of the treatment is due to insurance benefit issues. In fact brackets for orthodontics were dislodged due to carelessness by the patient. He does not want to pursue this mode of treatment. Either prior to or after implant placement, bone graft will be placed distally (Fig.1: in large amount (red circles)) and buccally (Fig.2 (coronal section). If primary stability is acceptable, an immediate provisional is fabricated. He will be traveling abroad soon.
If the (mesio)distal bone resorption is less (Fig.1), D2 implant may be appropriate.
Fig.3 is a PA taken 2 years preop, whereas Fig.4 immediately preop showing purulent discharge from the distal gingival sulcus (*). When the tooth is extracted, the socket is rounded, favoring placement of a rounded implant instead of D-shaped implant. The coronal opening of the socket is ~ 8x8 mm. Granulation tissue is removed from the buccal and distal aspects of the socket.
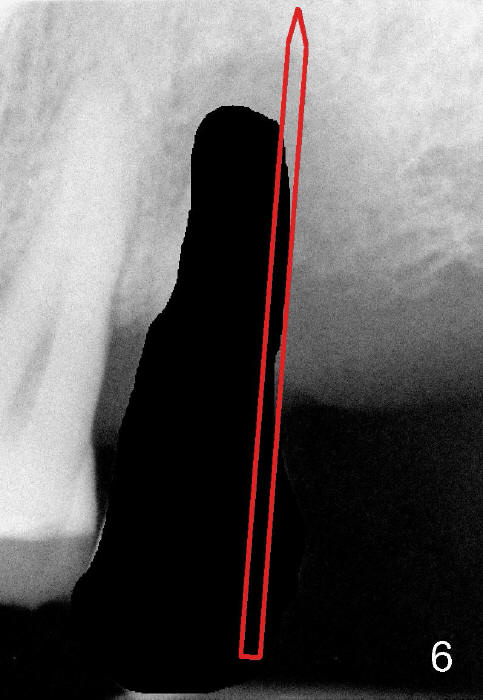
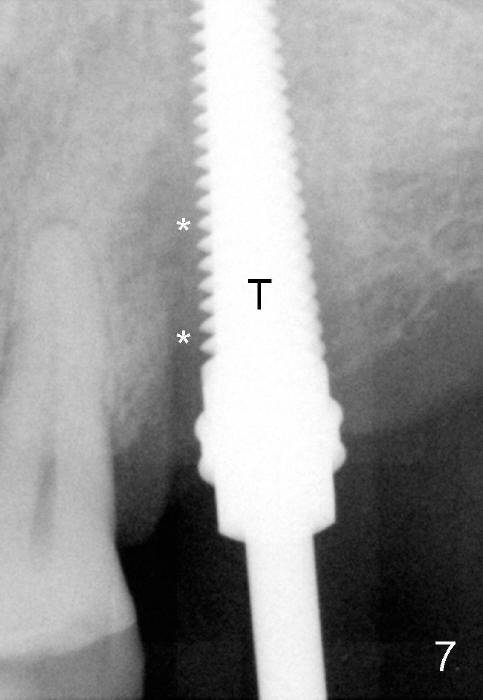
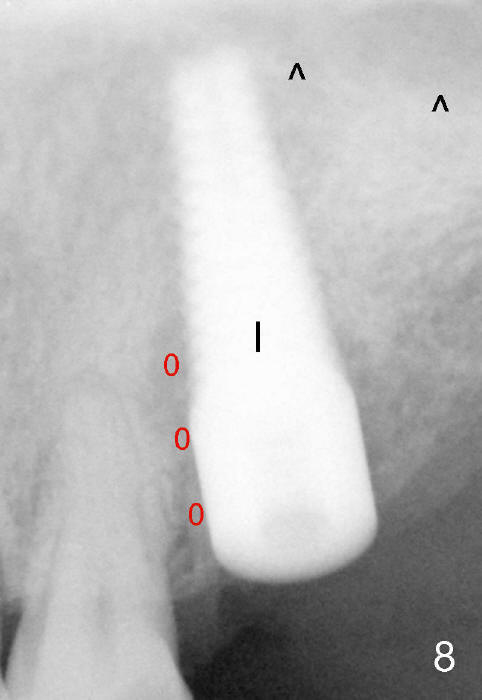
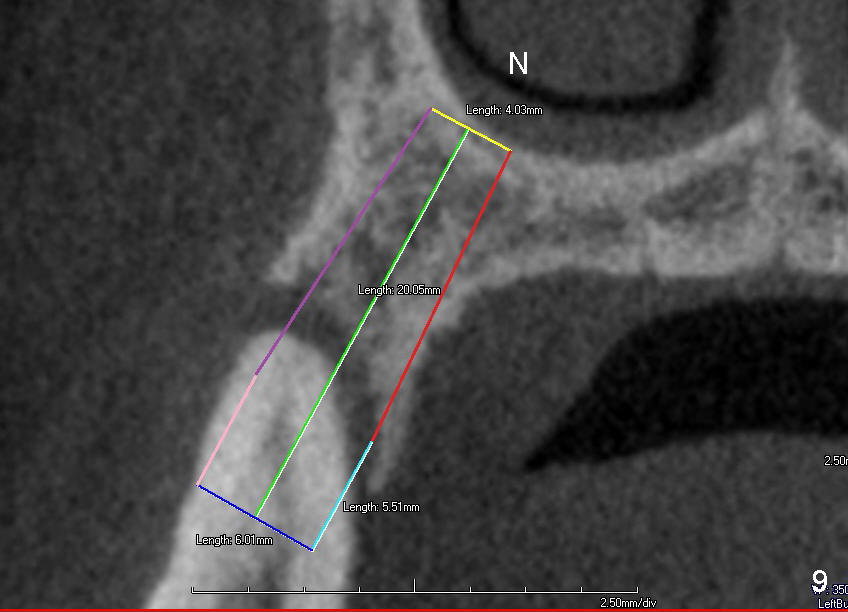
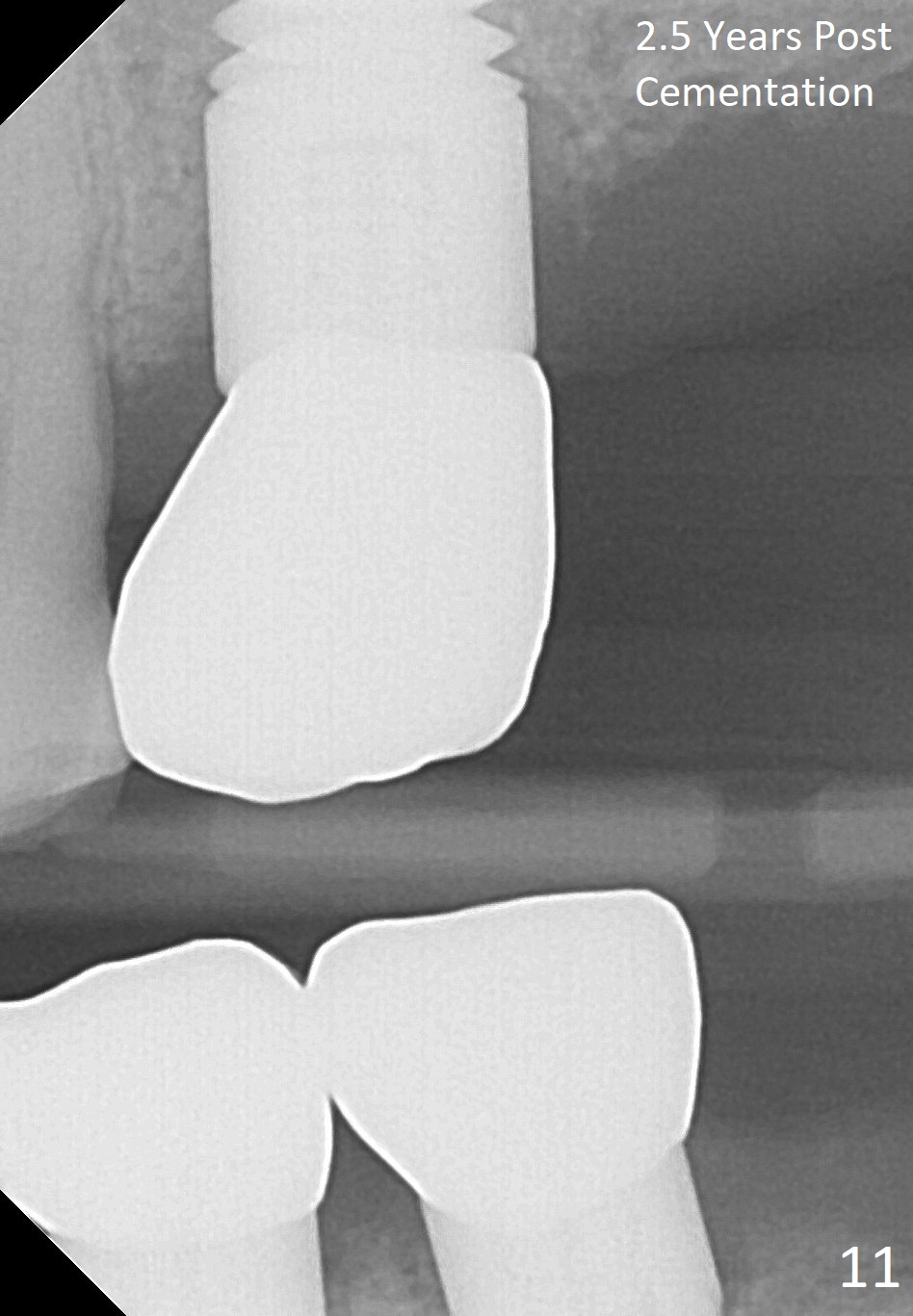
Fig.5 is an illustration showing the socket after extraction. The osteotomy is intentionally placed distally (Fig.6 arrow: pilot drill). In case the patient agrees to have ortho treatment, there will be space to correct the upper midline (7). If not, a molar crown will be fabricated. By the time a 4.5x20 mm tap is inserted (Fig.7 T), the mesial gap is visible (*). When a 6x20 mm implant is placed (Fig.8 I), bone graft is placed buccally (Fig.2, as planned) and mesially (Fig.8 red circles, as compared to Fig.1). The implant has to be as large and long as 6x20 mm to get primary stability (insertion torque 50/60 Ncm). The apex of the implant is close to the sinus floor (Fig.8 ^) or in fact the nasal floor (Fig.9 N). There appears bone growth in the mesial gap 3 months postop (Fig.10 *). There is no bone loss 2.5 years post cementation (Fig.11).
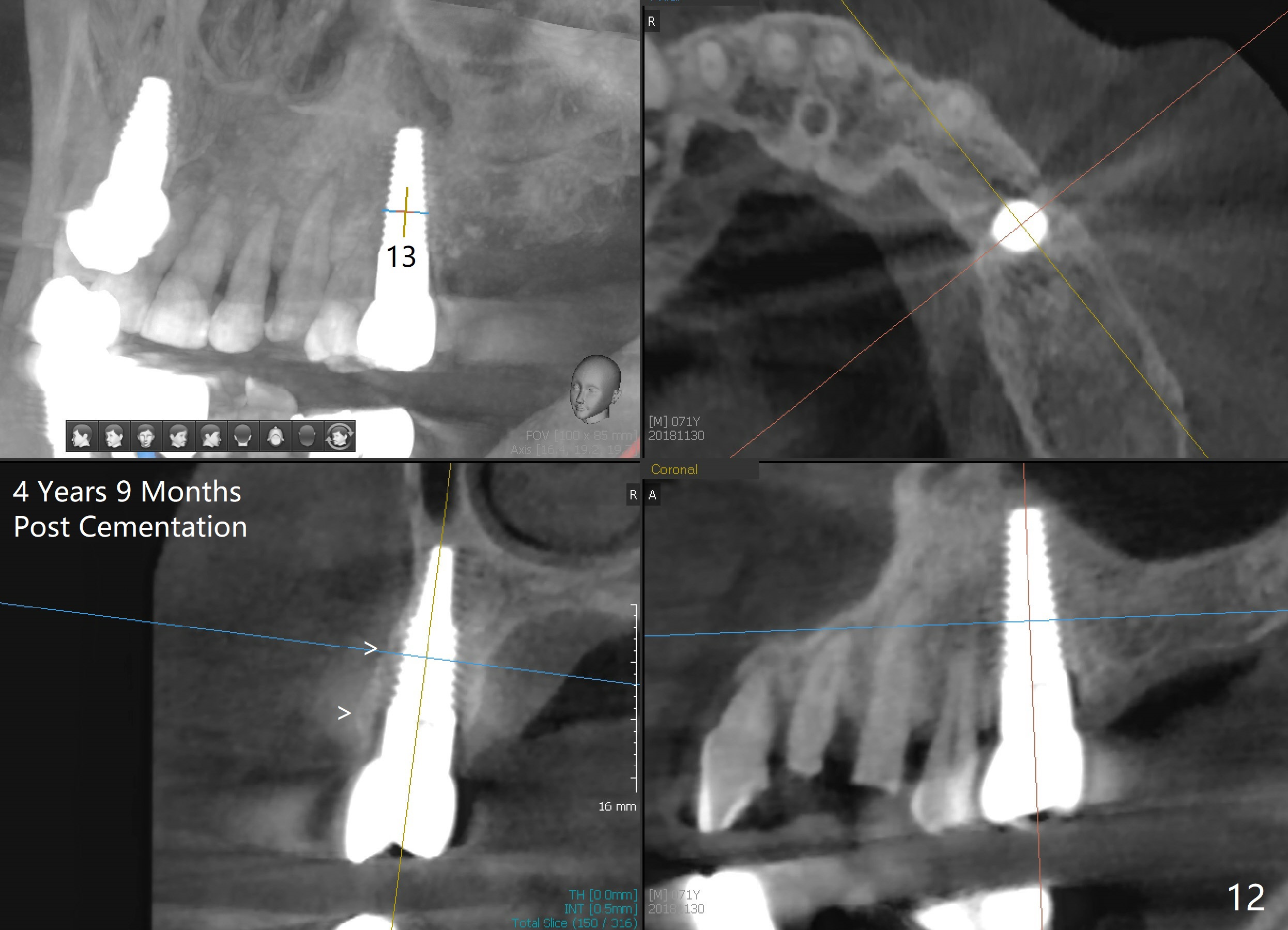
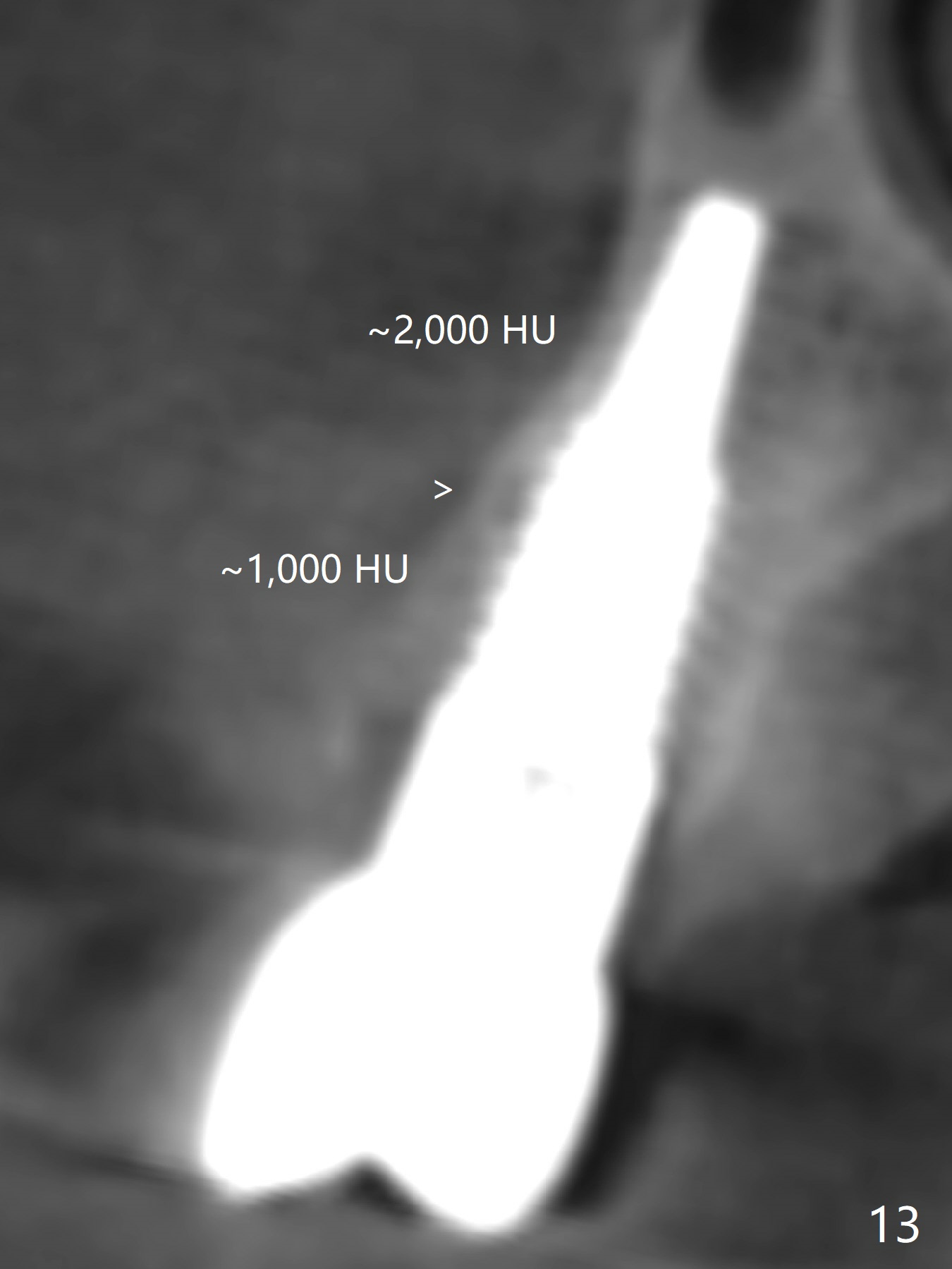
CT taken 4 years 9 months post cementation shows that the coronal portion of the buccal plate regenerates (Fig.12 between arrowheads, as compared to Fig.2,9). The density is ~1,000 Hounsfield Units, as compared to ~2,000 HU of the apical portion (Fig.13).
Return to Upper Arch and Full Mouth Reconstruction,
Immediate Implant for Upper Bicuspids,
Implants & Ortho
Xin Wei, DDS, PhD, MS 1st edition 12/21/2014, last revision 12/17/2018