





.jpg)


|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|
||
|
|
|
|
|||
|
|
|
|
|
||
|
|
|
|
|||
Atrophic Ridge & Staged Provisionalization 一段式植体5年随访
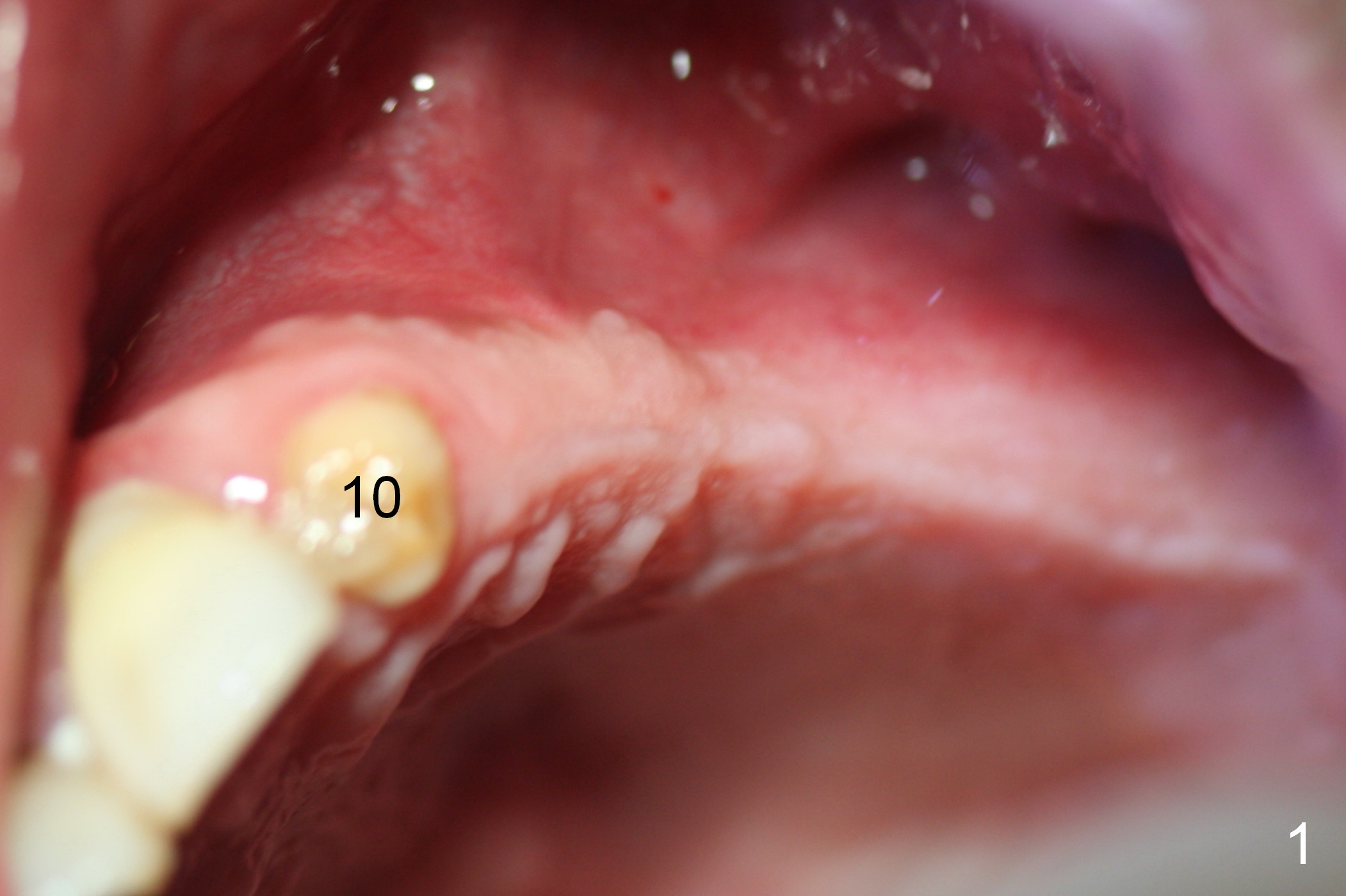
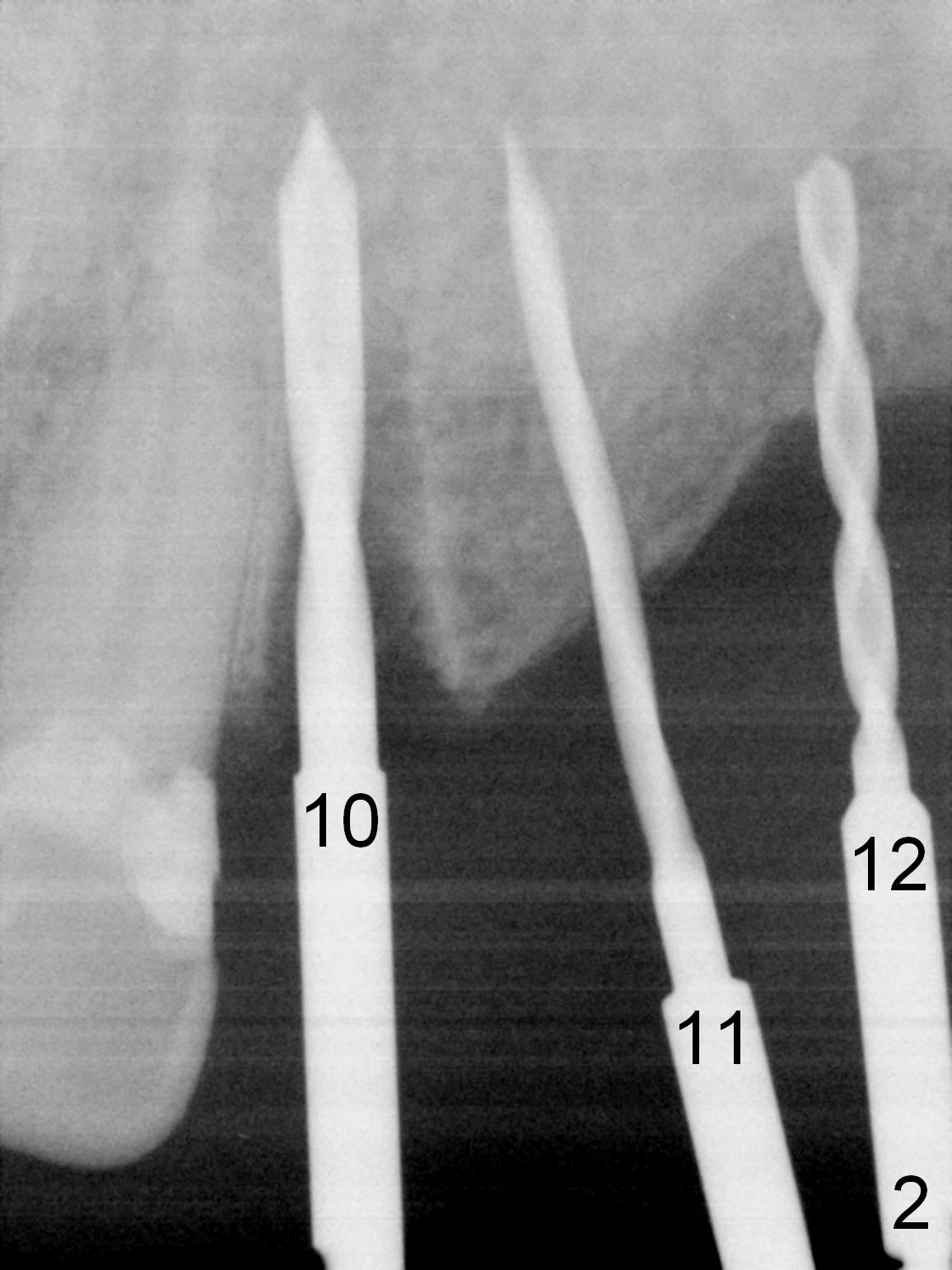
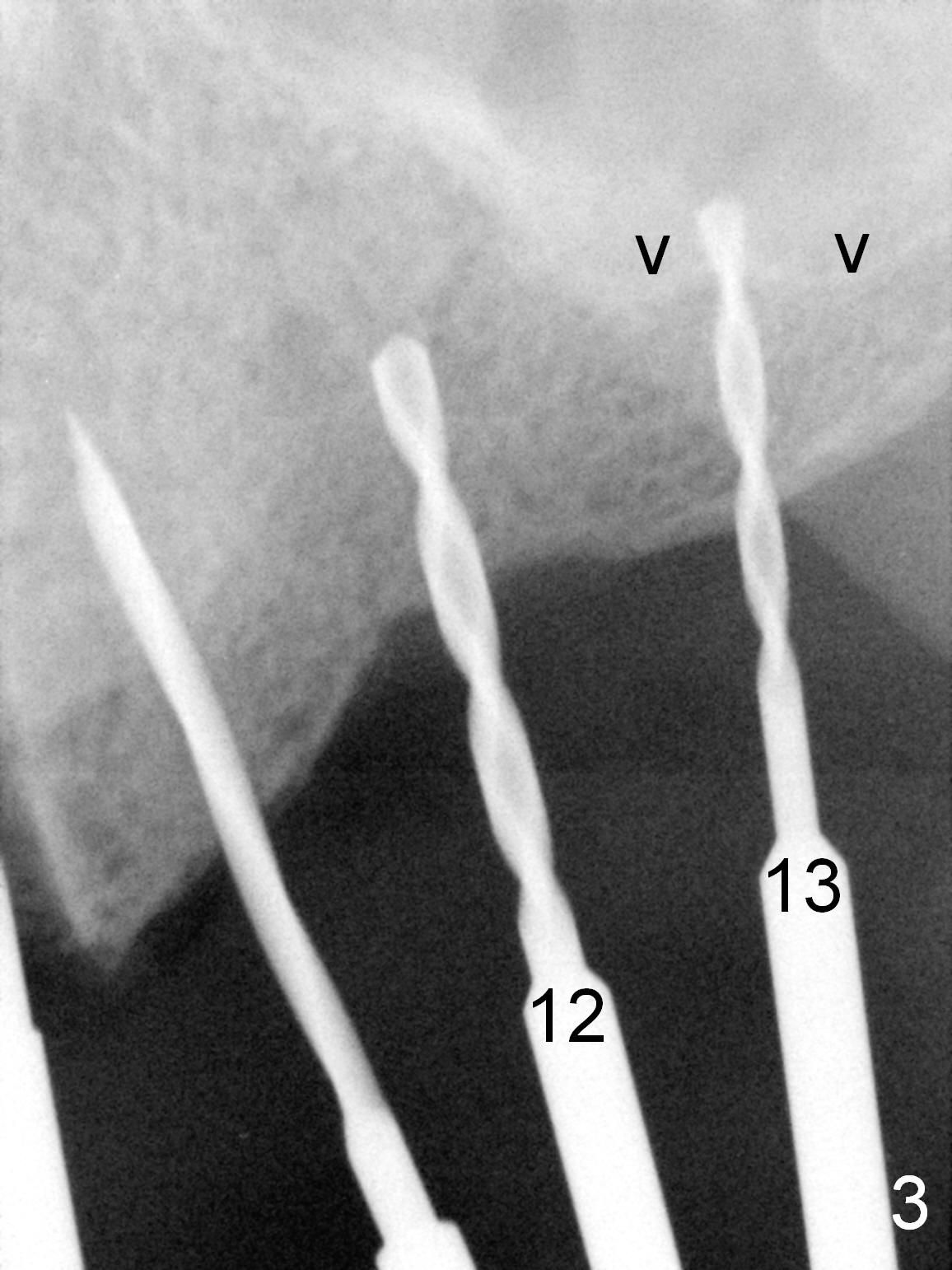
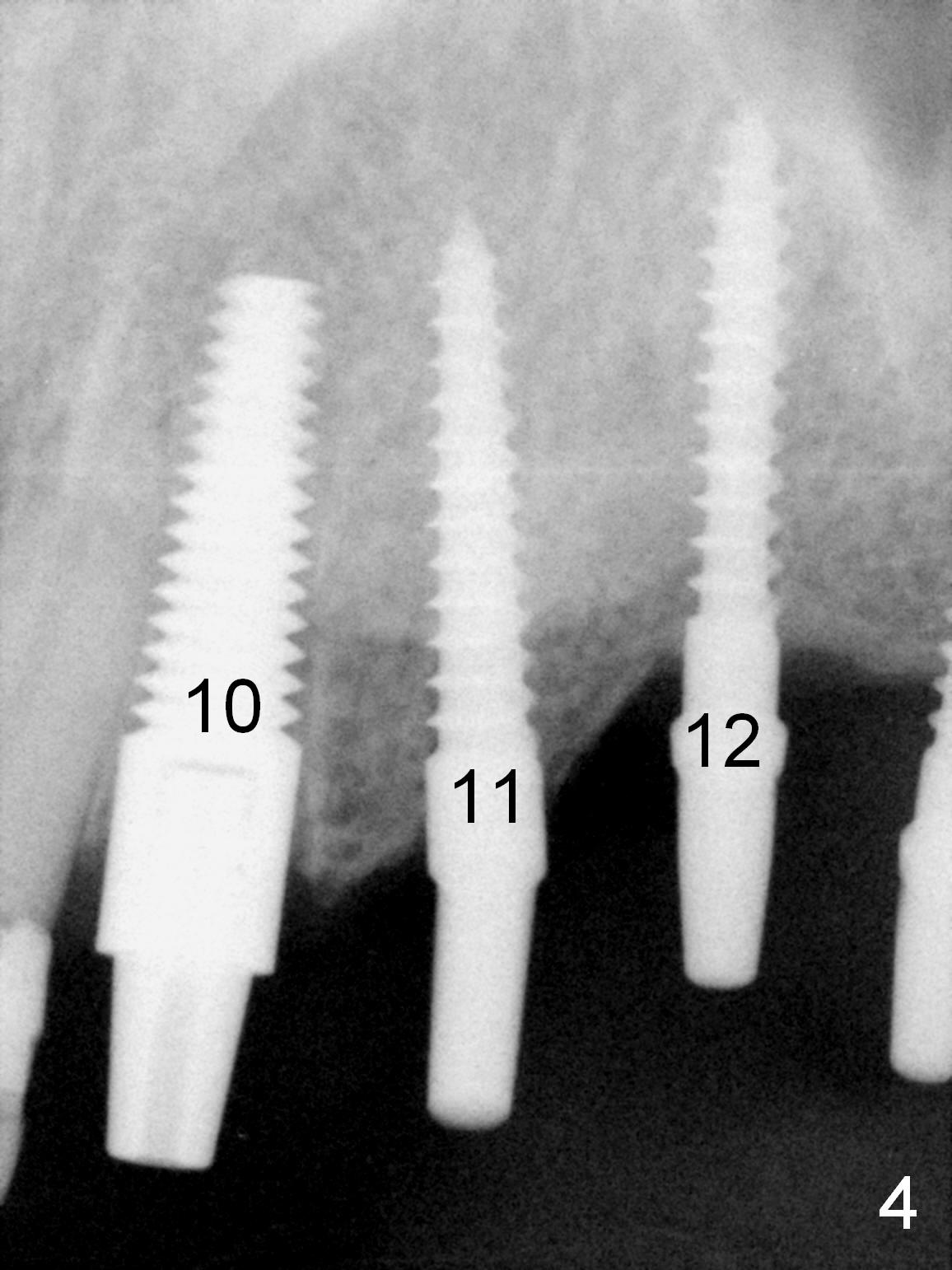
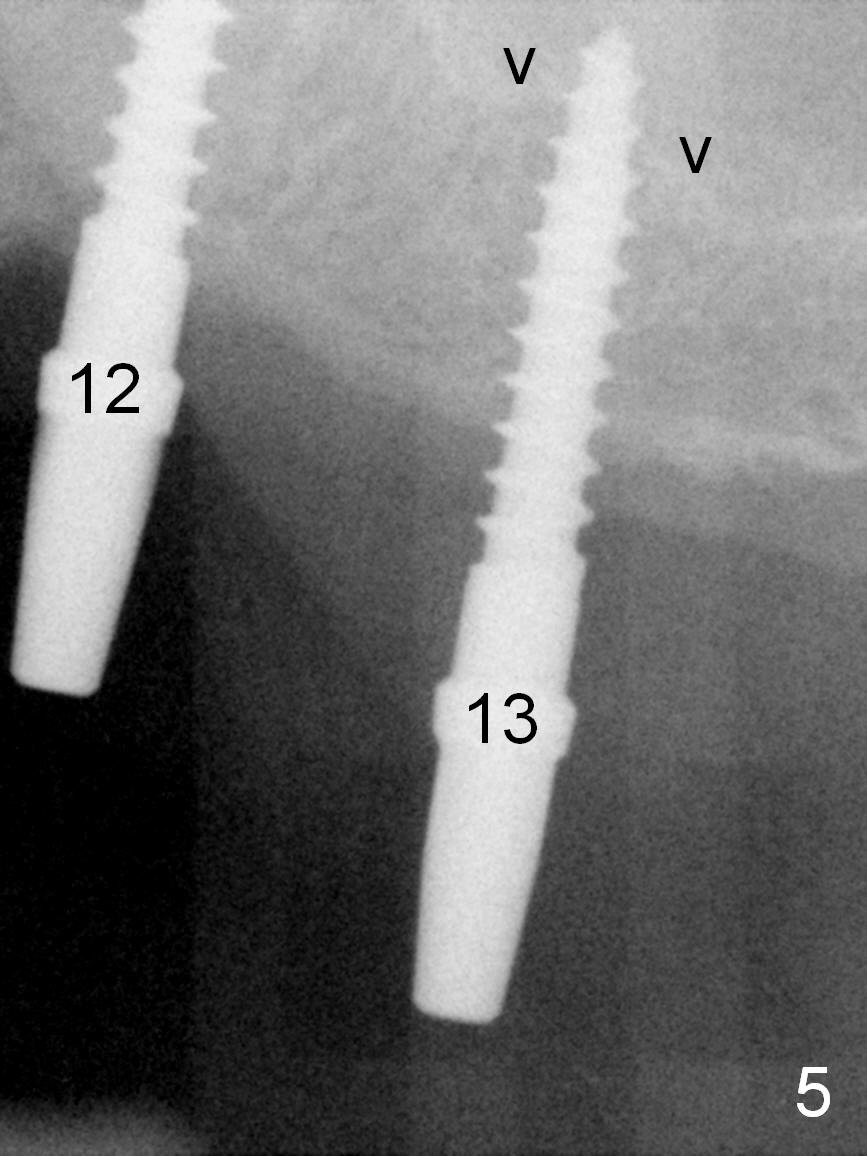
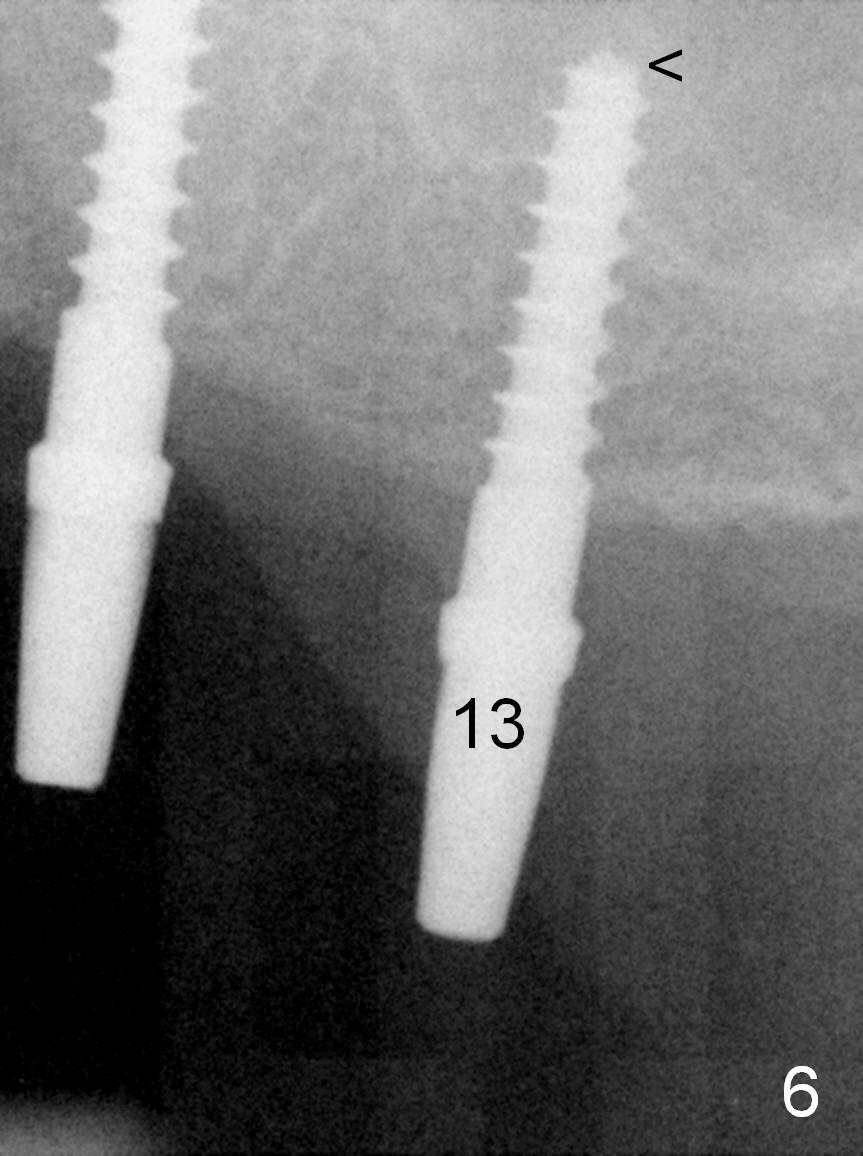
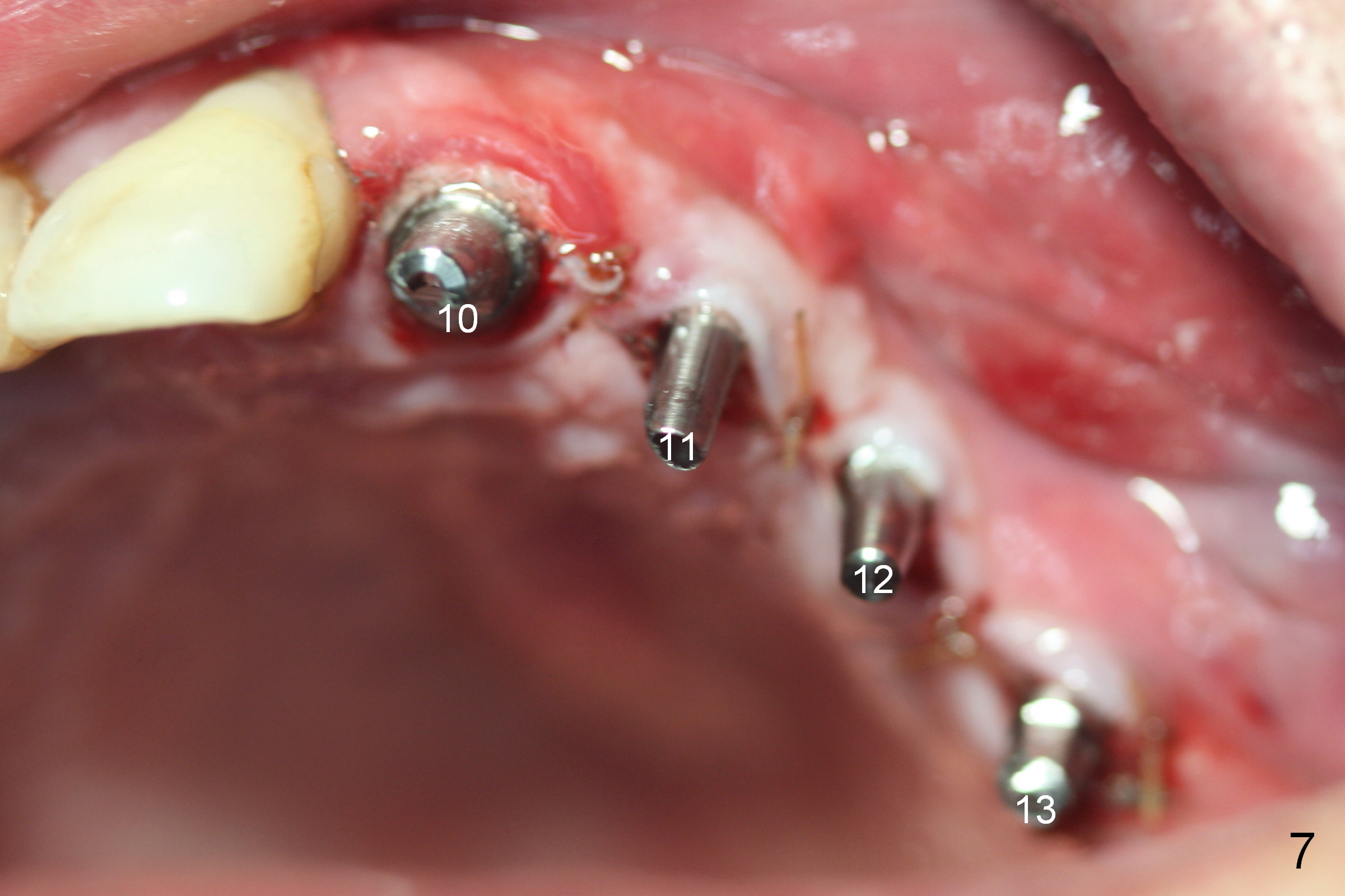
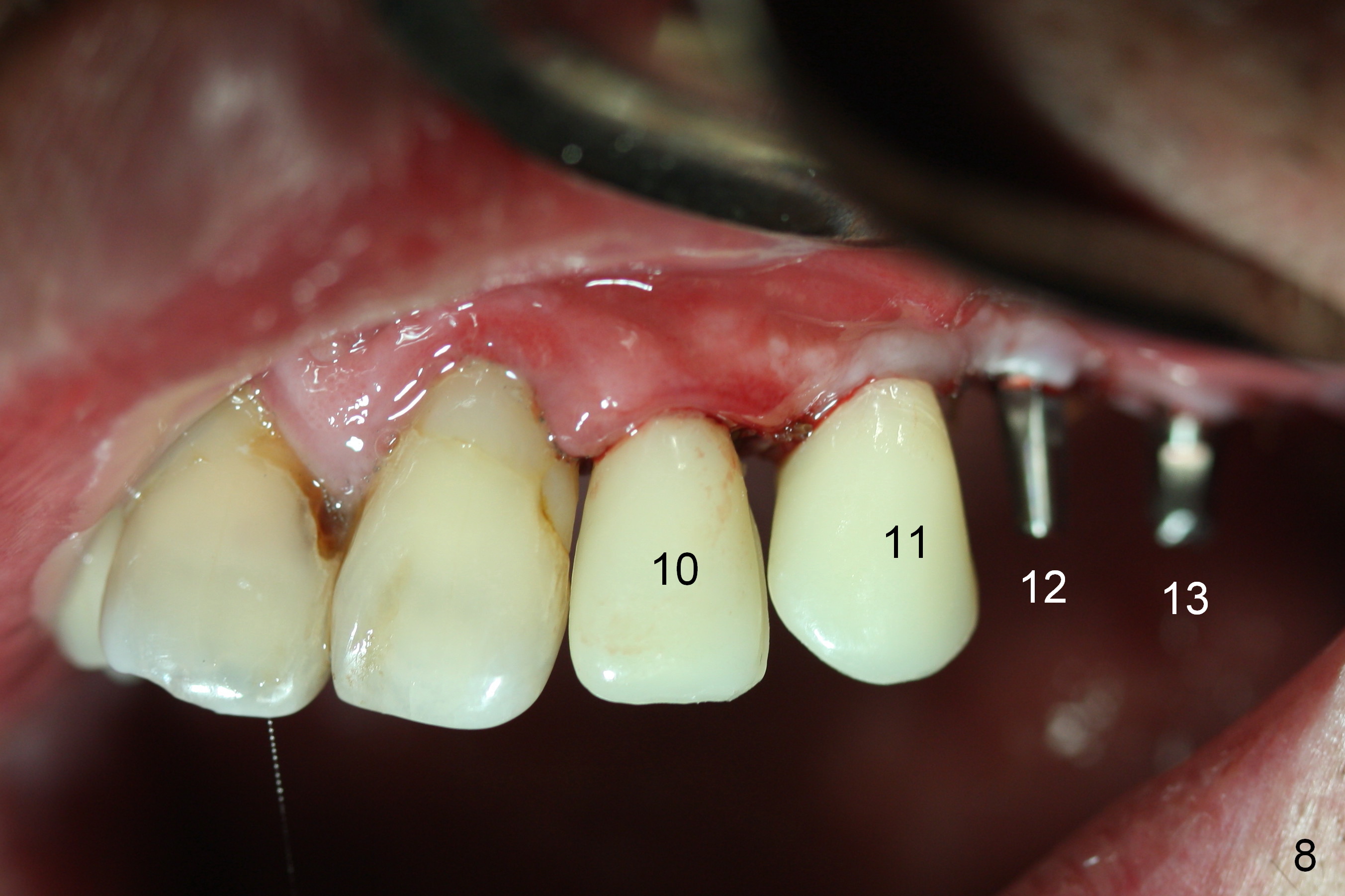
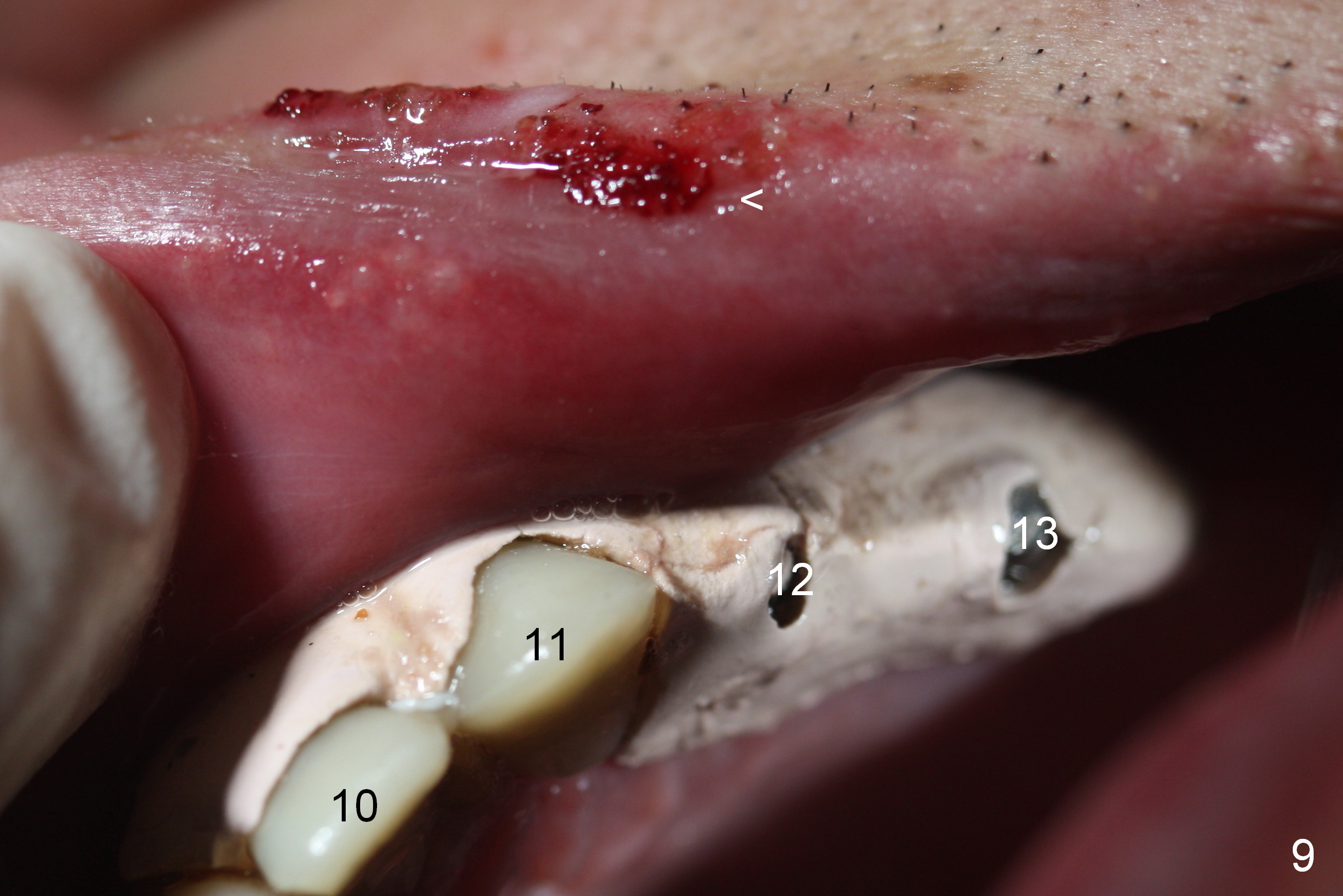
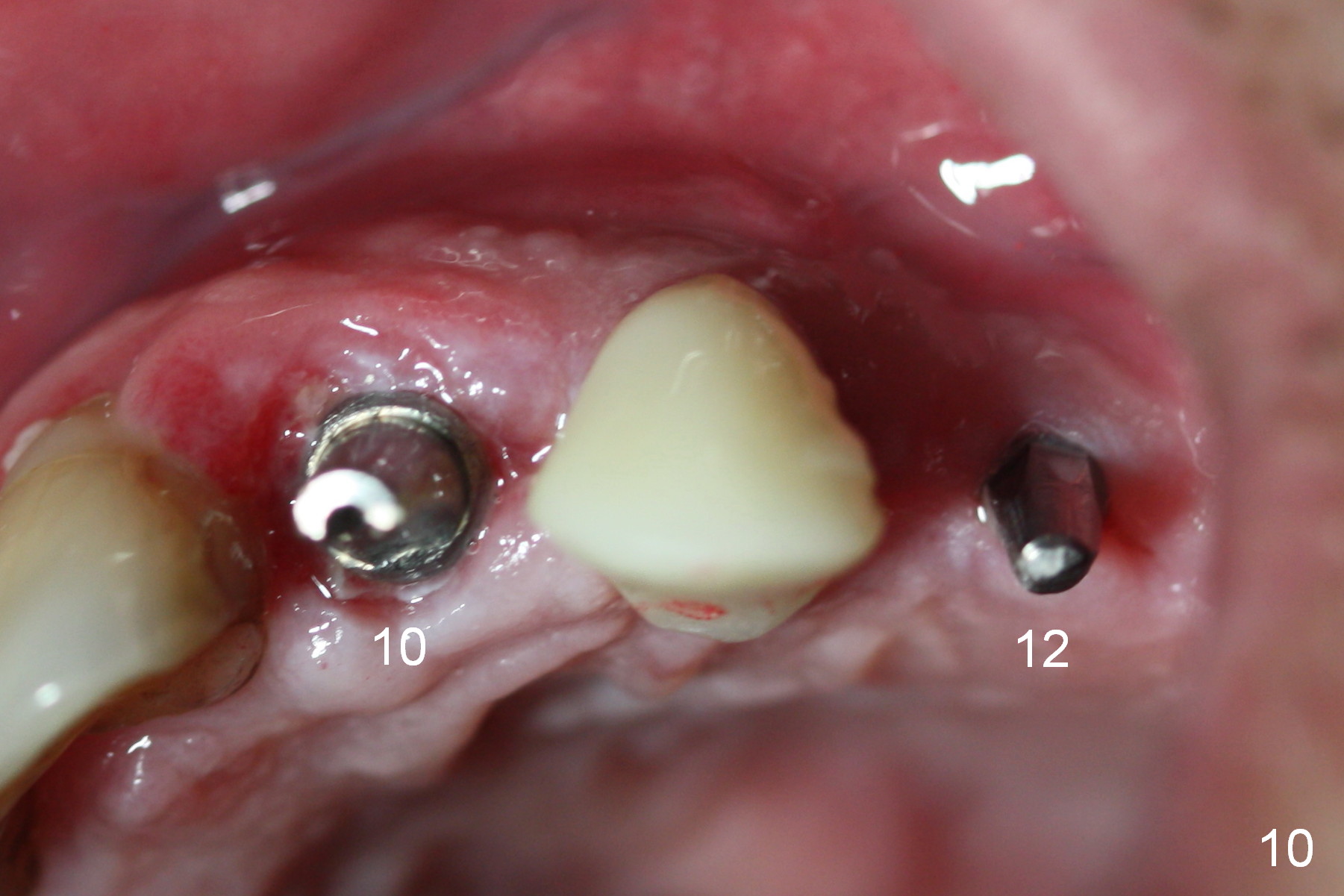
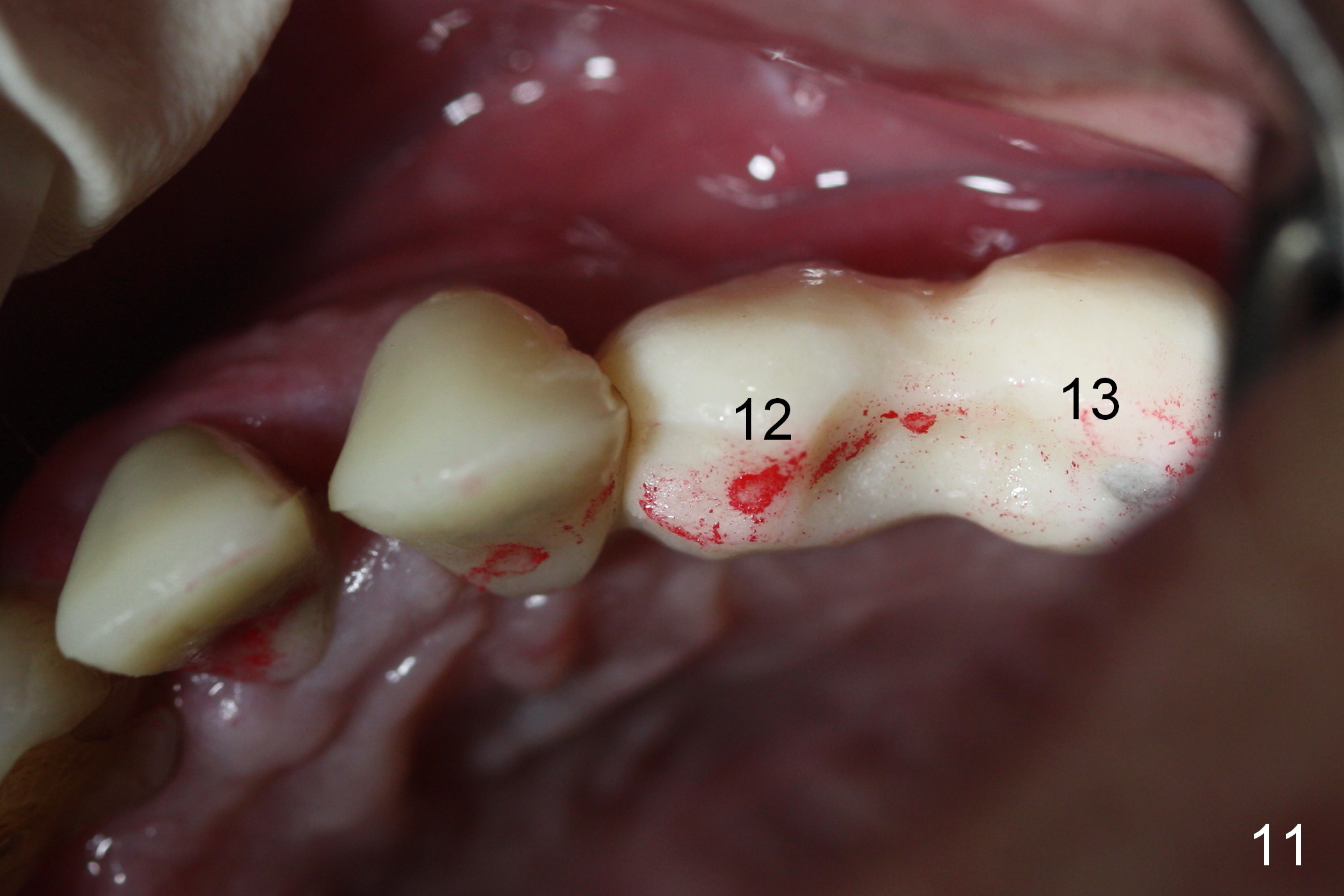
When the patient returns for implant placement (2nd visit after initial exam), he reveals that he is a dental phobic. He requests placement of 4 implants in the upper left quadrant, instead of 2. Narrow ridge is unexpected in the canine and premolar area (Fig.1). Limited bone height at #13 (Fig.3 arrowheads: sinus floor) is found when initial drills are in place (Fig.2,3). A 2-piece implant (4.5x17 mm tissue-level) is placed at #10 after extraction, while 1-piece implants are placed at 11 (3x17 mm (tissue-level, 15 °) and 12 and 13 (bone-level, 2.5x14, 12 mm, respectively; Fig.4,5). In fact the 1 piece implant at #13 is not completely placed (Fig.5). It is removed, the apical 3 threads are cut off (Fig.6 <, since a shorter implant was unavailable in the office) and the remaining implant is re-inserted. The insertion torques of the 4 implants are ~ 60, ~ 35, < 35 and 15 Ncm, respectively. After adjustment (Fig.7), immediate provisionals are fabricated at #10 and 11 (Fig.8, later splinted with composite), while perio dressing is applied around the implants at #12 and 13 and the provisionals at #10 and 11. There is no nasal hemorrhage postop. Although the perio dressing is loose 1 week postop (Fig.9), it is not removed. When the upper lip fissure (Fig.9 <) heals, provisionals at #12 and 13 are planned to be splinted to the other two ones. Two weeks postop, the upper lip fissure heals, the perio dressing dislodges and the implants at #12 and 13 are stable (Fig.10). After abutment height adjustment, a splinted provisional is fabricated over these 2.5 mm 1-piece implants (Fig.11).
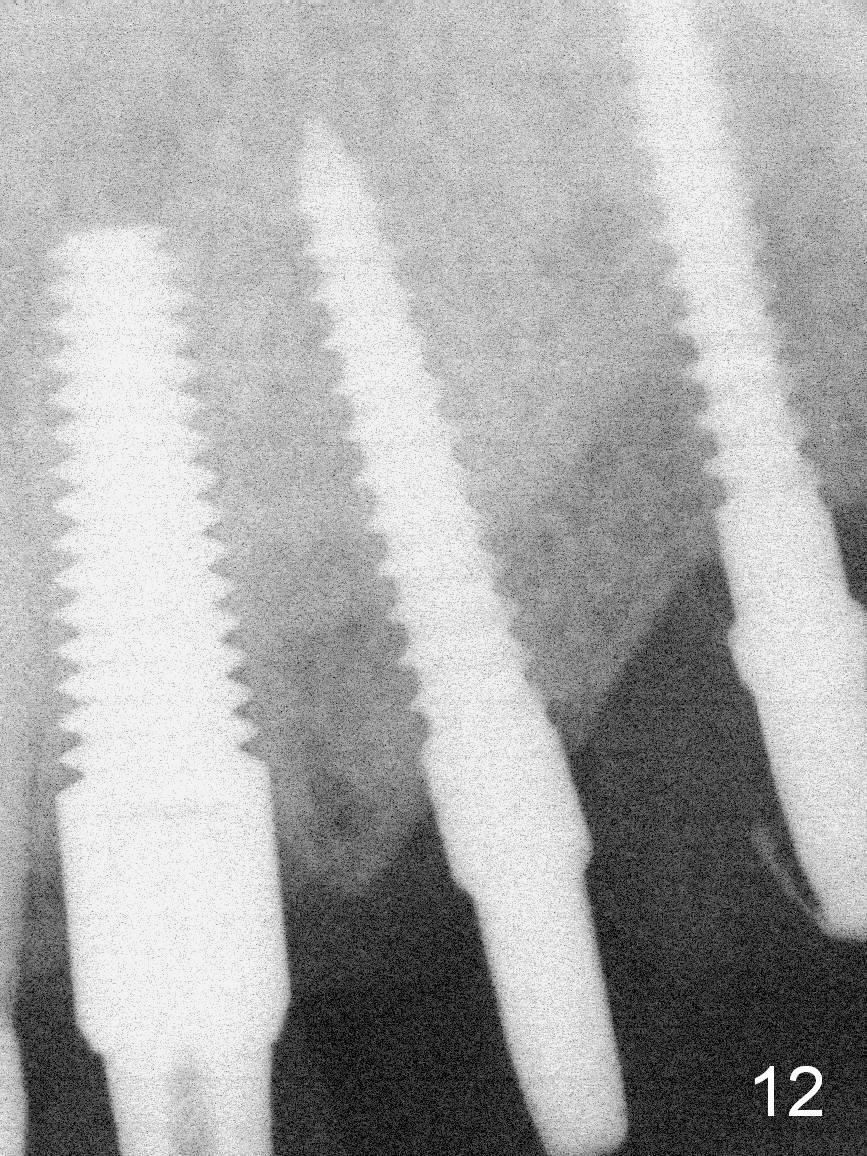
The patient returns for final restoration 3.5 months postop; it appears that the implants have osteointegrated (Fig.12,13). After reprep, there is no gross buccal plate atrophy at #10 (Fig.14).
At the time of cementation, the crowns at #11-13 do not contact the gingiva (Fig.16). One month post cementation, the gingiva appears to have grown coronally (Fig.17).
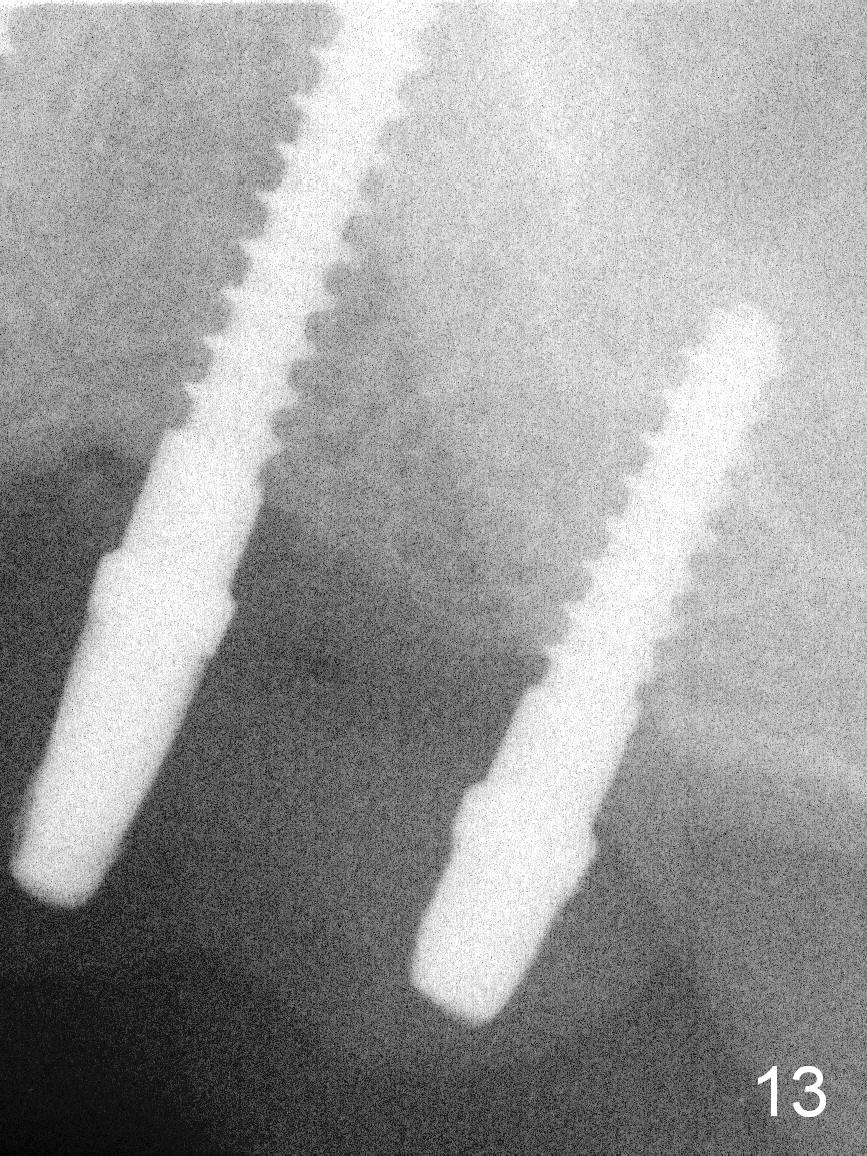
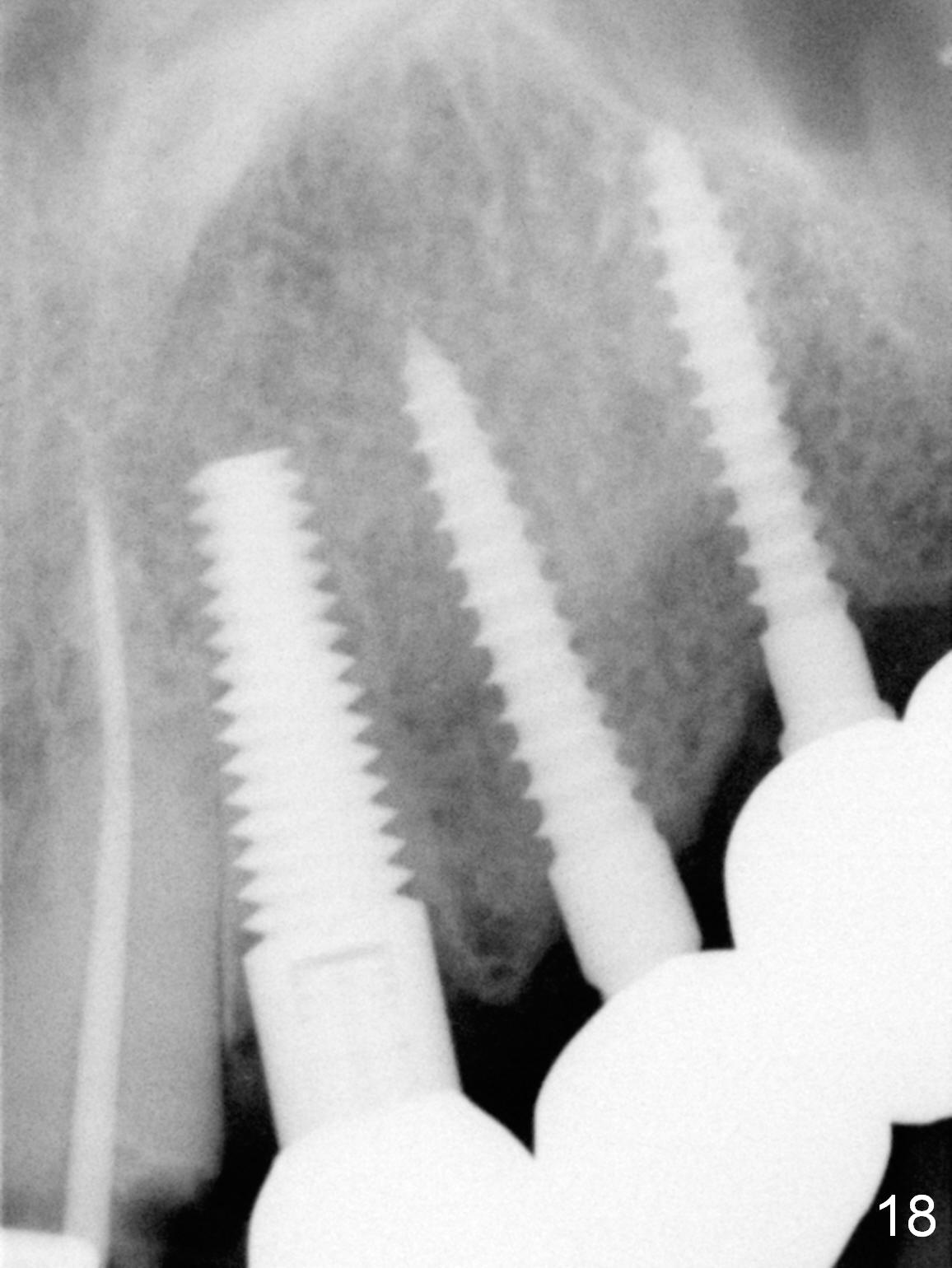
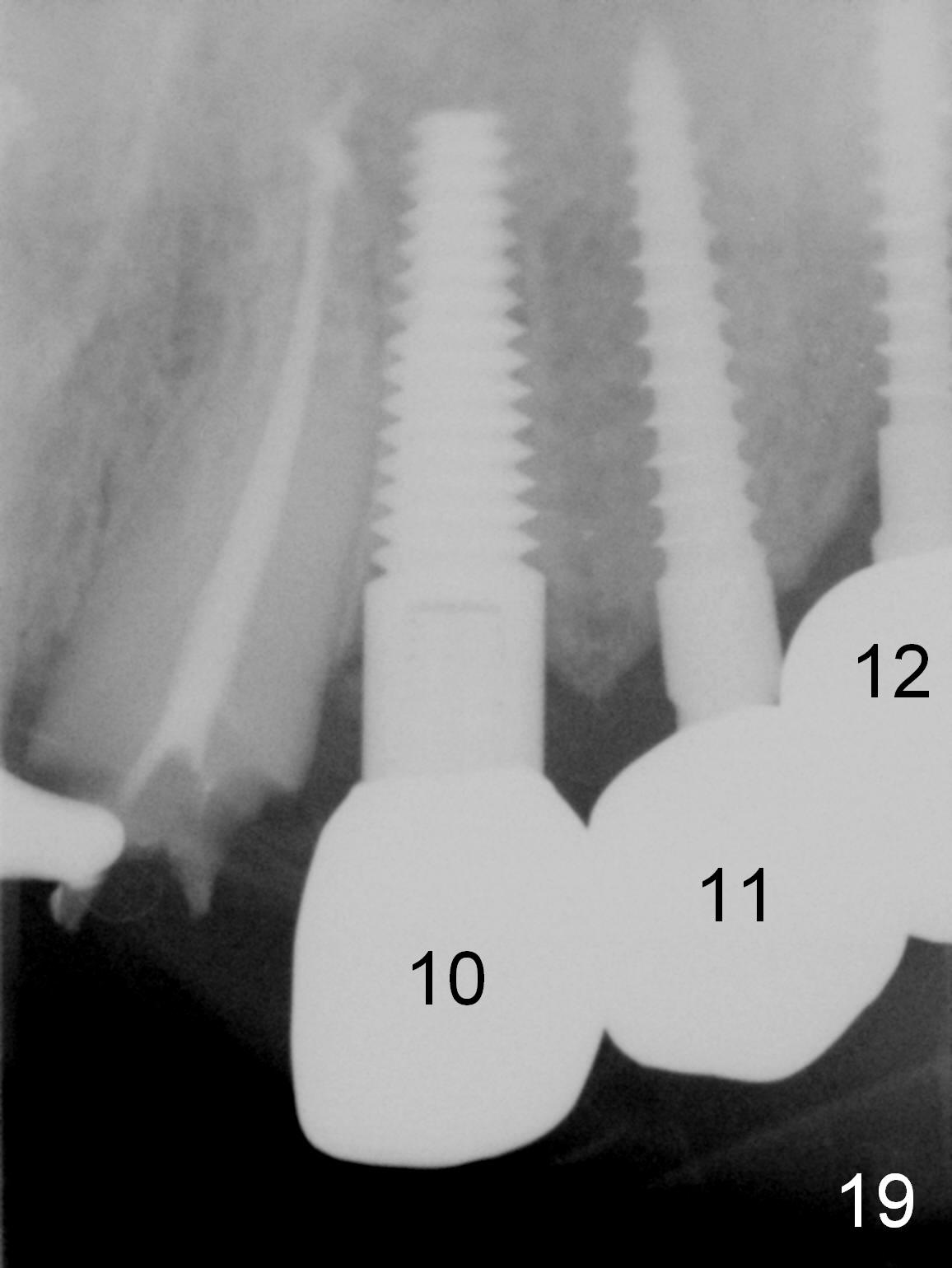
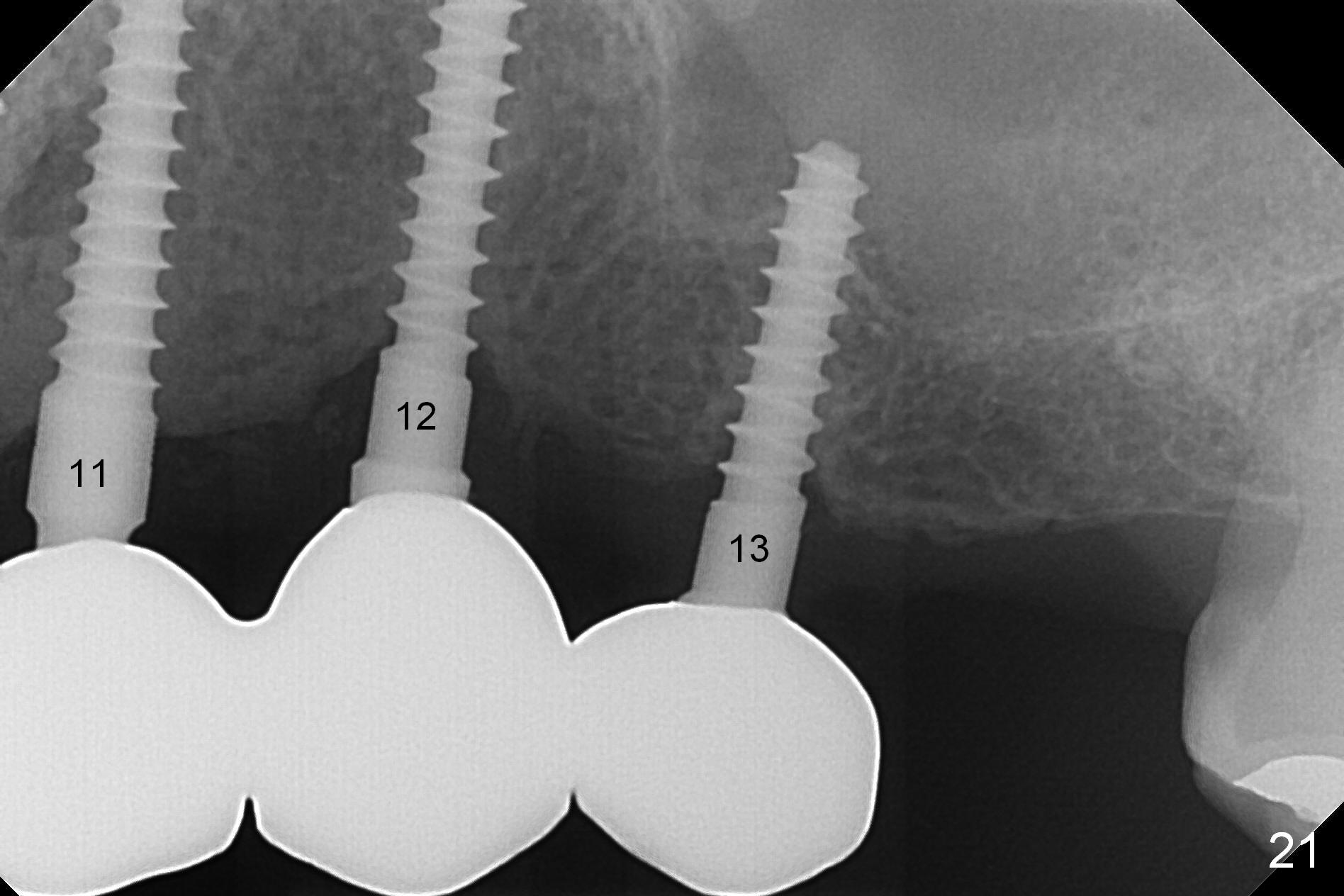
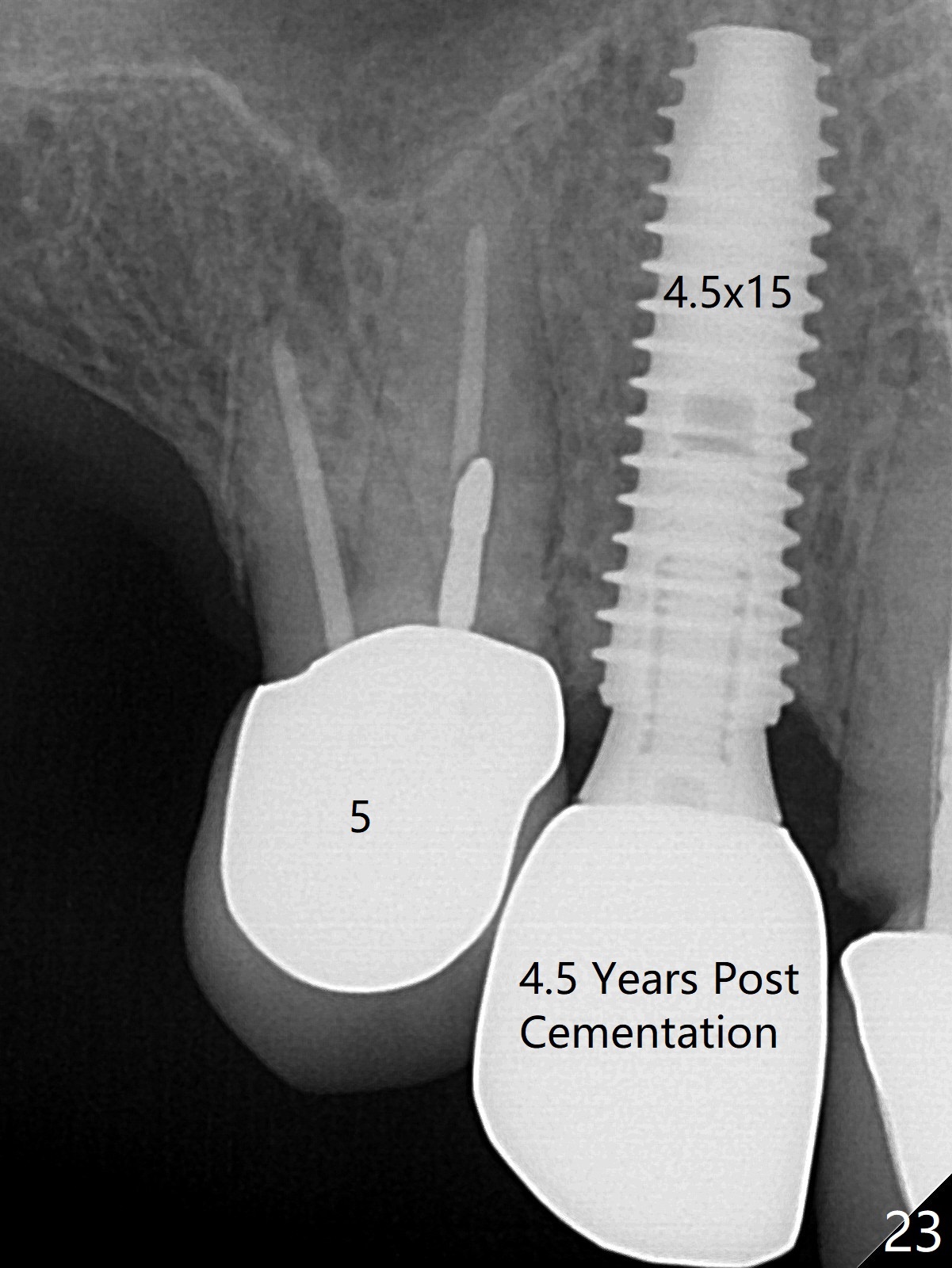
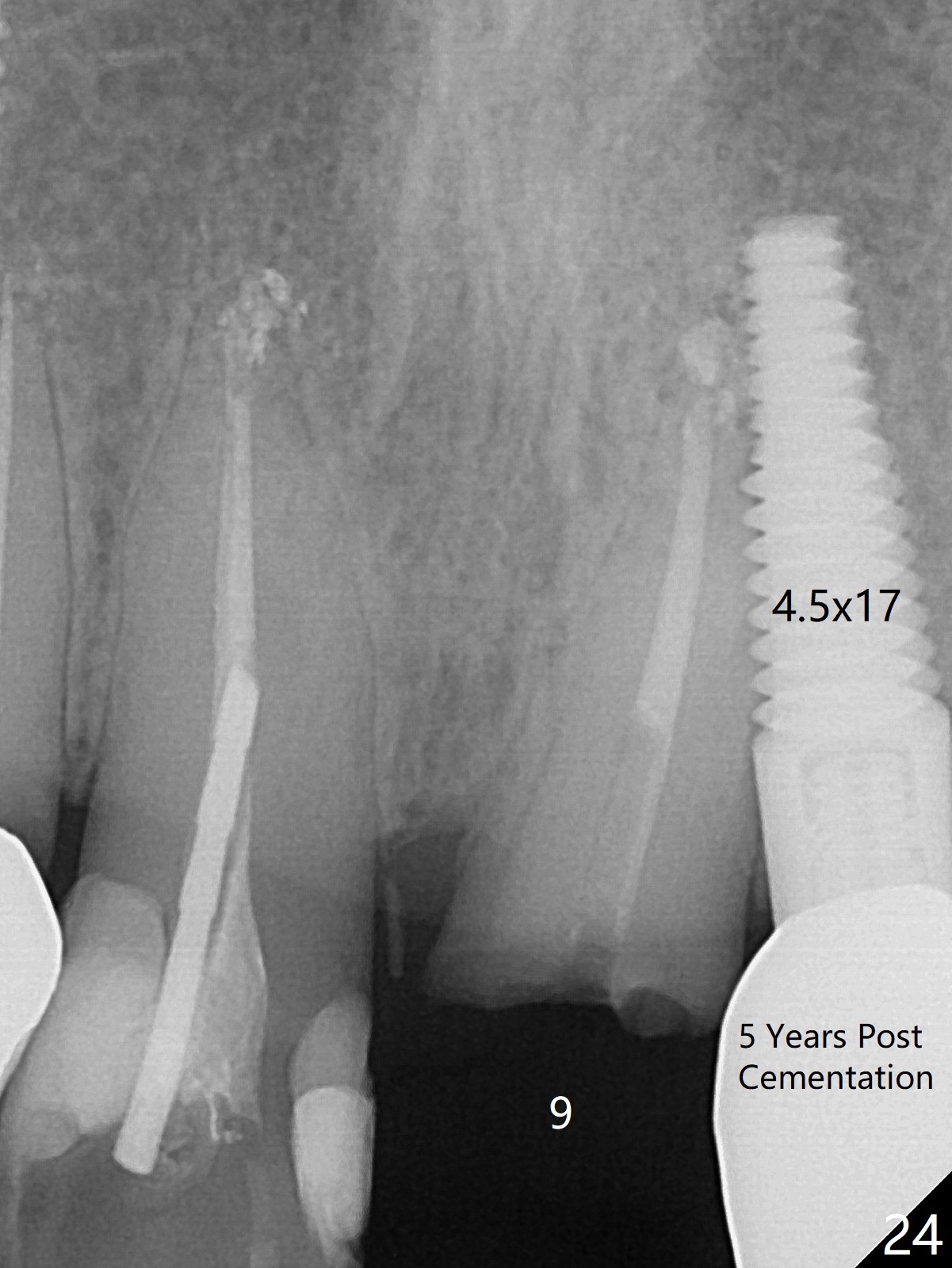
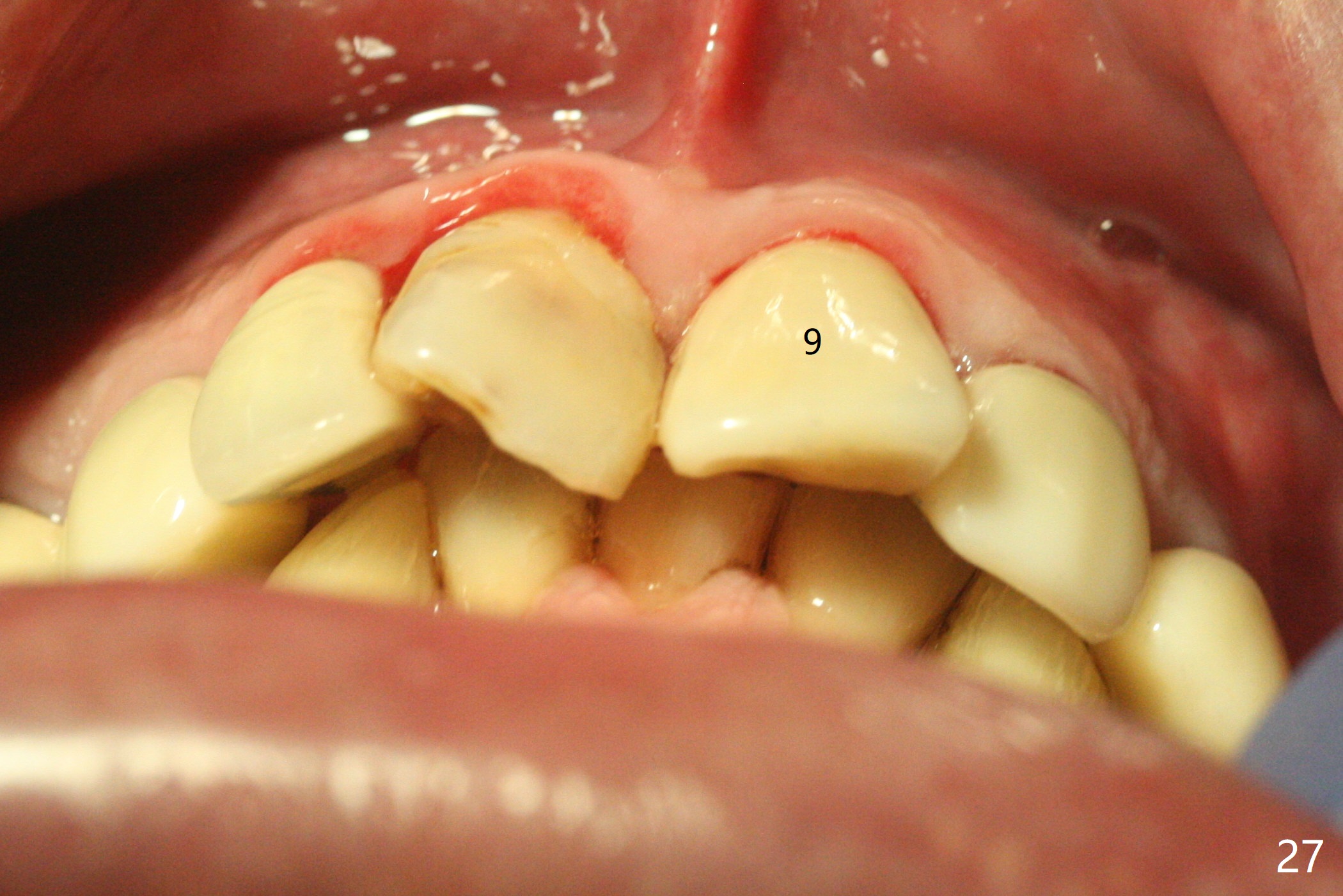
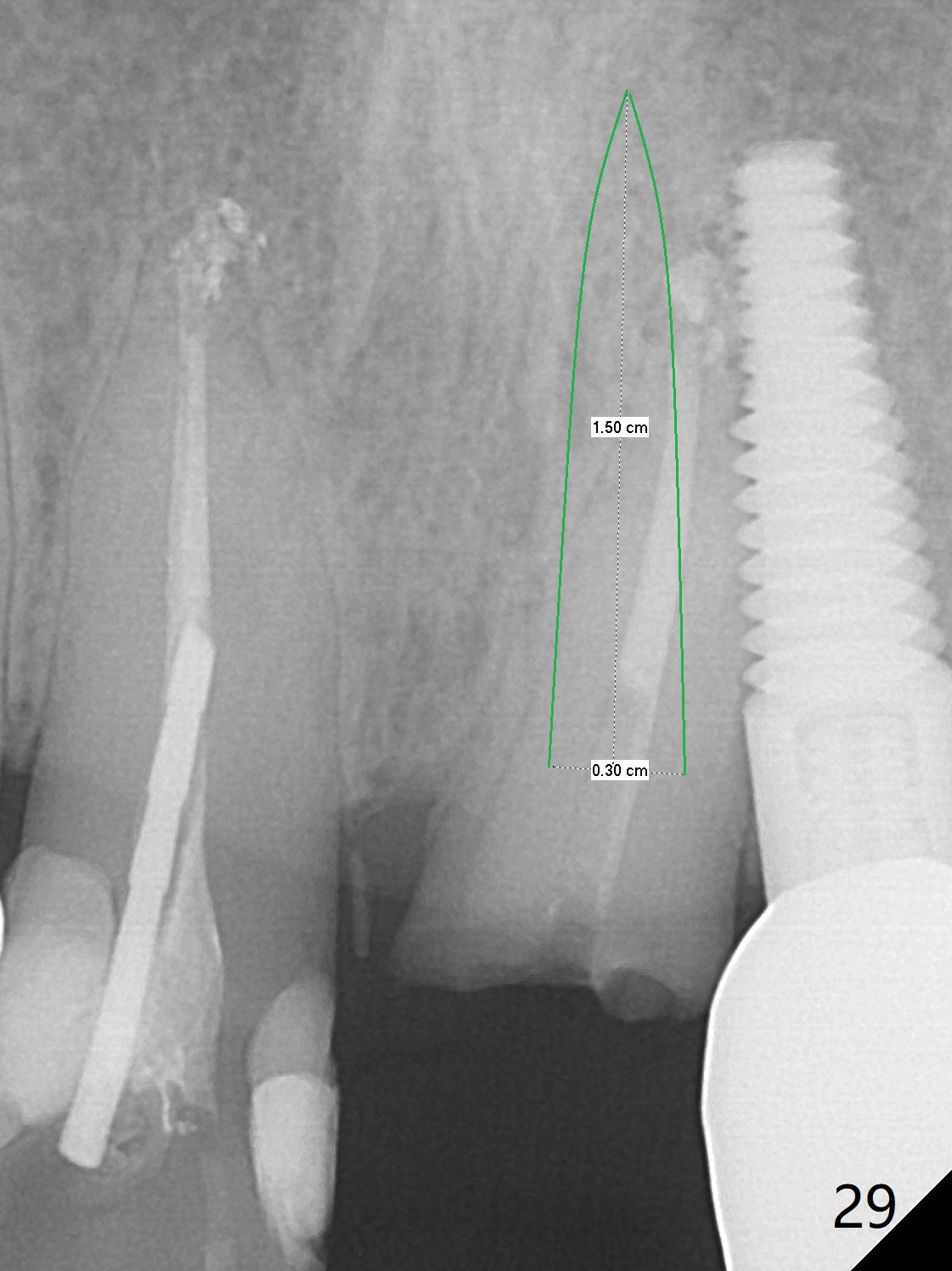
Six months post cementation, the tooth #9 becomes symptomatic. Is it possible that the implant at #10 is too close to the root of #9? It is asymptomatic after pulpotomy, but the tooth fractures equi/supragingivally. Two PAs taken while RCT show osteointegration at #10-12 (Fig.18,19). While the bone density increases at #10 regular implant, there is minimal bone loss around the 1-piece implants 13 months post cementation (18 months postop, Fig.20,21). The gingiva remains healthy 19 months post cementation (Fig.22). 76岁病人突然打电话说一个植牙牙冠松动,其实9号牙(自然牙)折裂,6,10-13号牙植牙好像没有骨质吸收(图二十三至二十五),10-13牙位牙龈健康(图二十六,行使功能五年)。9号牙牙冠重新粘固后,显示前牙深覆合,深覆盖(图二十七,二十八)。如果再次脱落需要植牙,选择一段式有助于植入和修复,因为植体和基台直径小。两段式植牙相对基台直径至少4,或者4.5毫米,前牙修复显得笨重。由于9,10牙根和植体接近,9号牙植体需要偏小而长,3x14或者15毫米(图二十九)。
Return to
Upper
Incisor Immediate Implant,
Upper Arch Immediate Implant,
Posterior Immediate Provisional,
Technicians,
Atrophic Ridge
Clindamycin
Protect
Graft
Xin Wei, DDS, PhD, MS 1st edition 09/27/2015, last revision 05/24/2021