
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
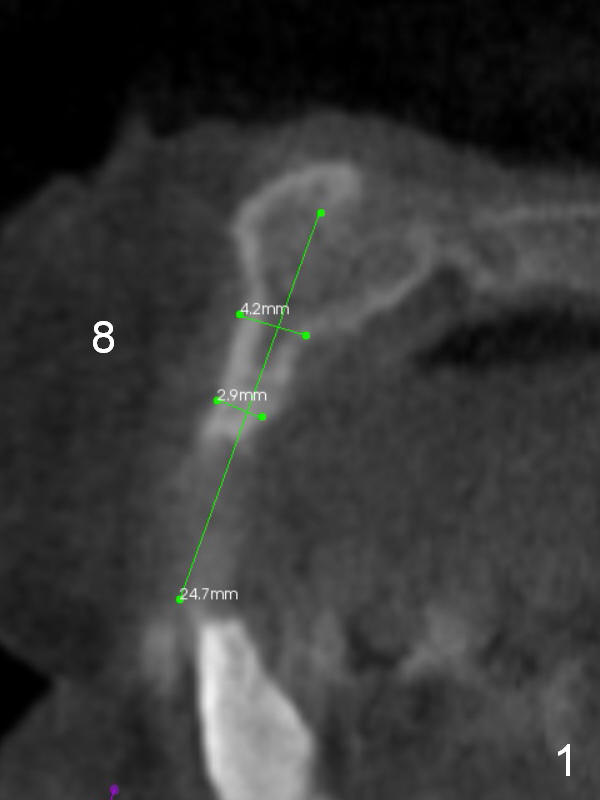
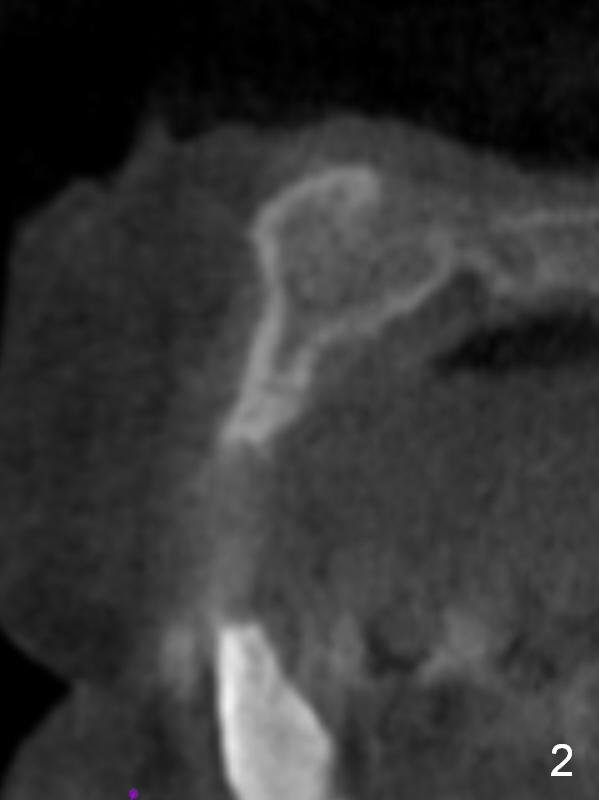
Atrophic Anterior Maxillary Ridge
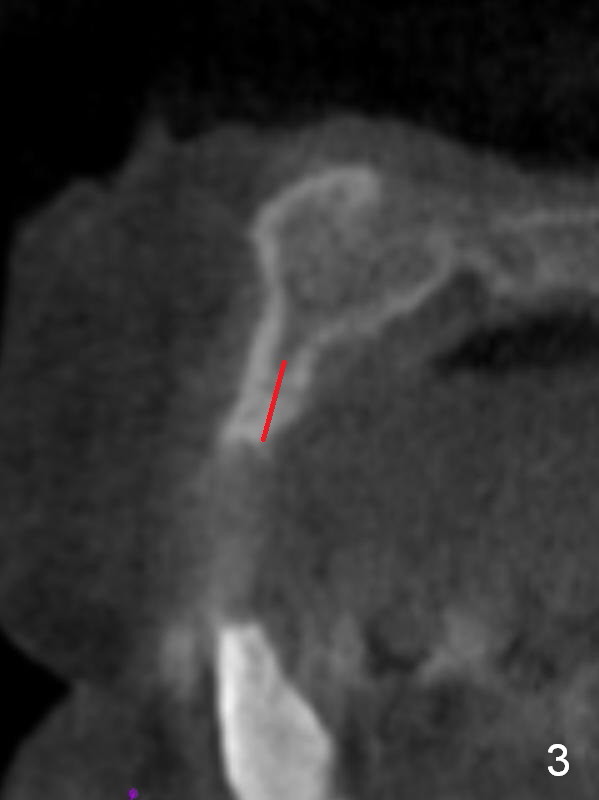
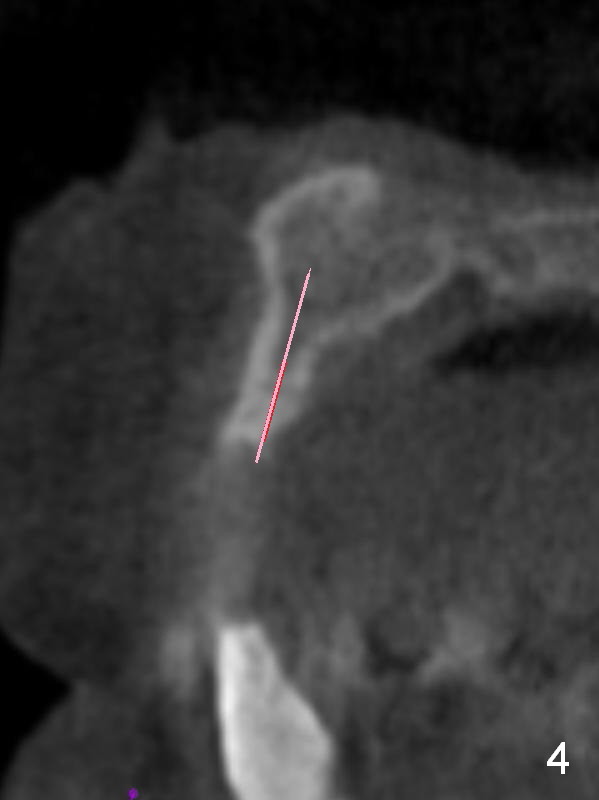
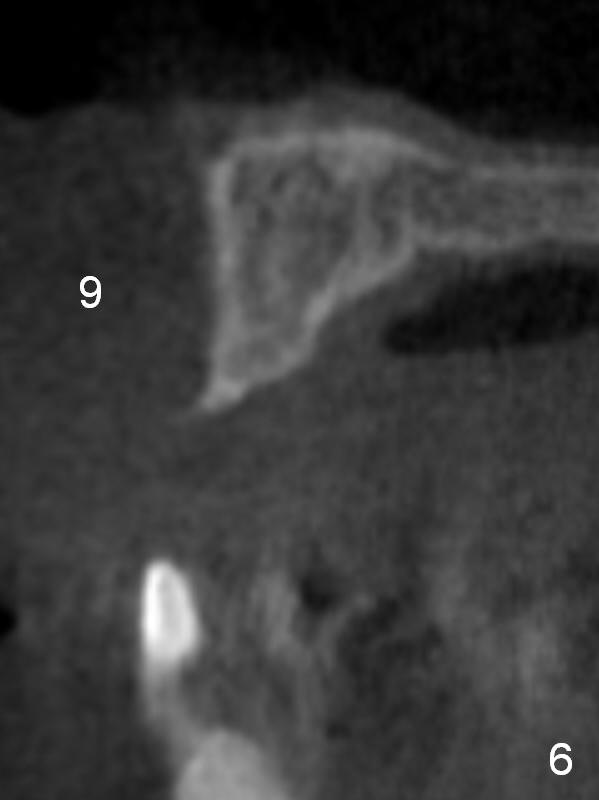
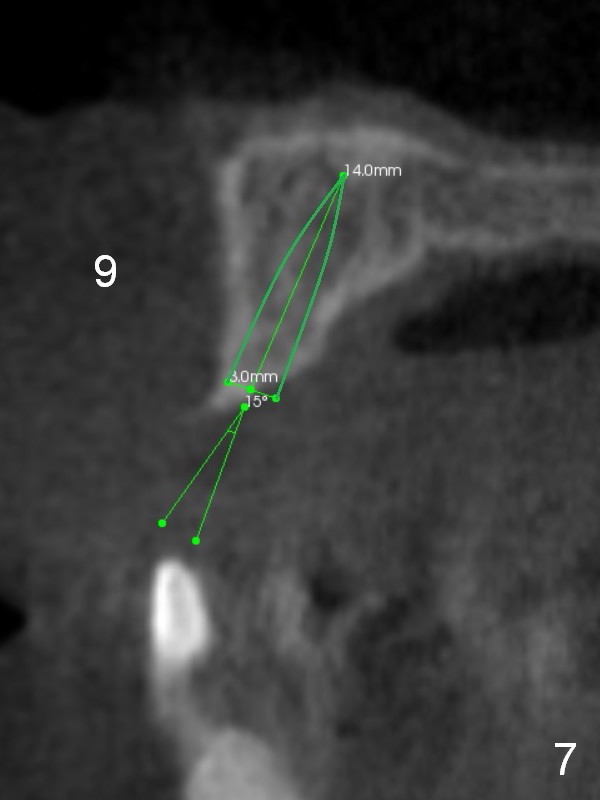
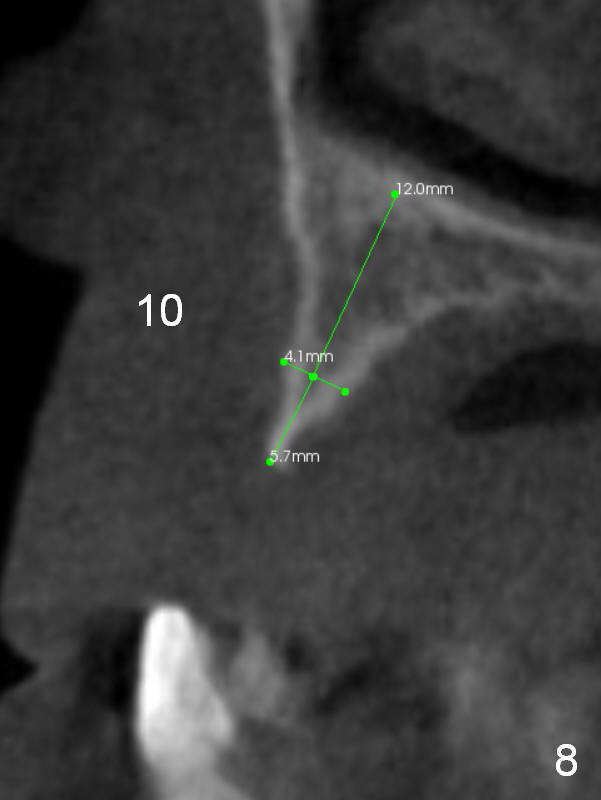
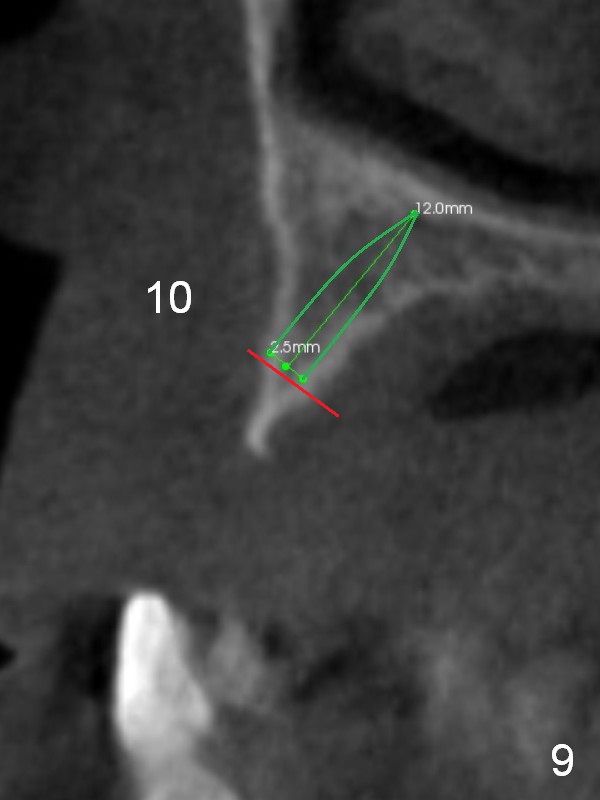
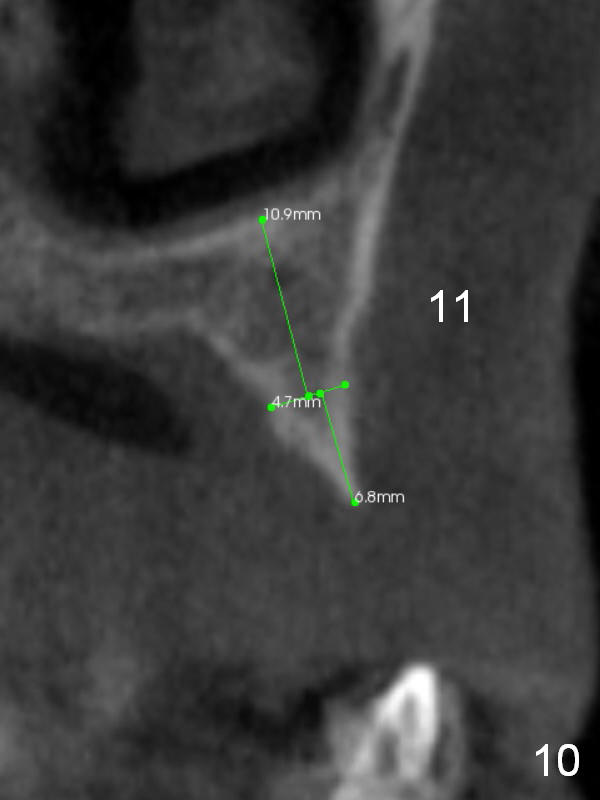
After implant reconstruction of the lower right and left (including #19) regions, the same treatment is considered in the atrophic anterior maxilla (#8-13) for anchorage for upper left molar cross bite correction. The smallest implants are to be placed in the each of the sites with different strategies. For example, at the site of #8 (Fig,1,2), ridge split with wheel (Fig.3) and microsteotomes (Fig.4) are used to place 1-piece implant (3x14 mm). The site of #9 has a pointed ridge and a wide base (Fig.6); a 1-piece angled implant (3x14 mm 15 °) is placed palatally (Fig.7). The ridge and base at #10 are narrow (Fig.8); after truncating the pointed ridge, a 2.0 or 2.5 mm 1-piece implant is placed parallel to the palatal wall (Fig.9).
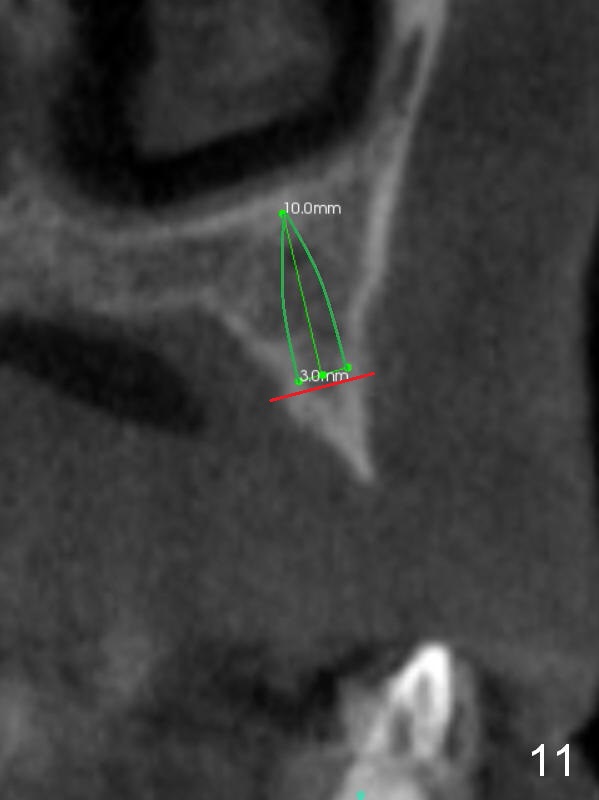
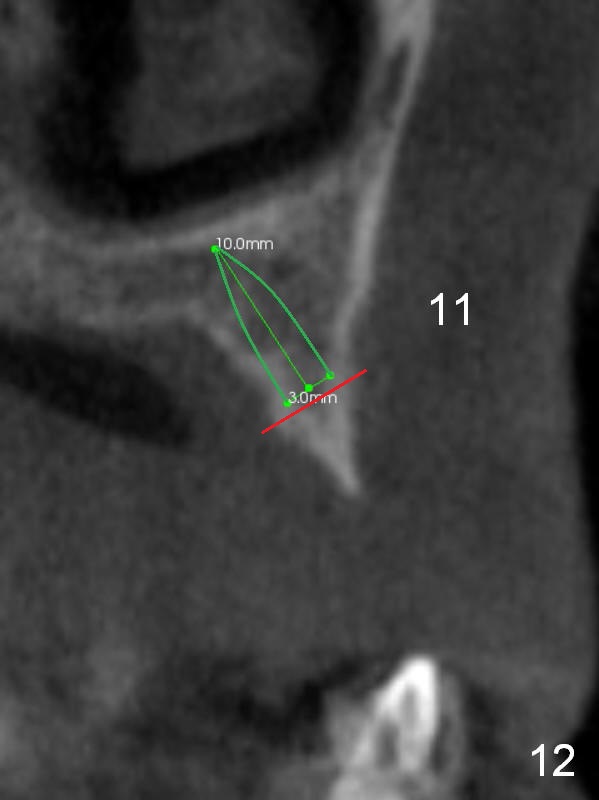
The ridge at #11 is similar to that at #10 (Fig.10), the treatment modality is the same (Fig.11,12). Comparison of the last 2 figures show that implant placement parallel to the palatal wall results in better trajectory for restoration.
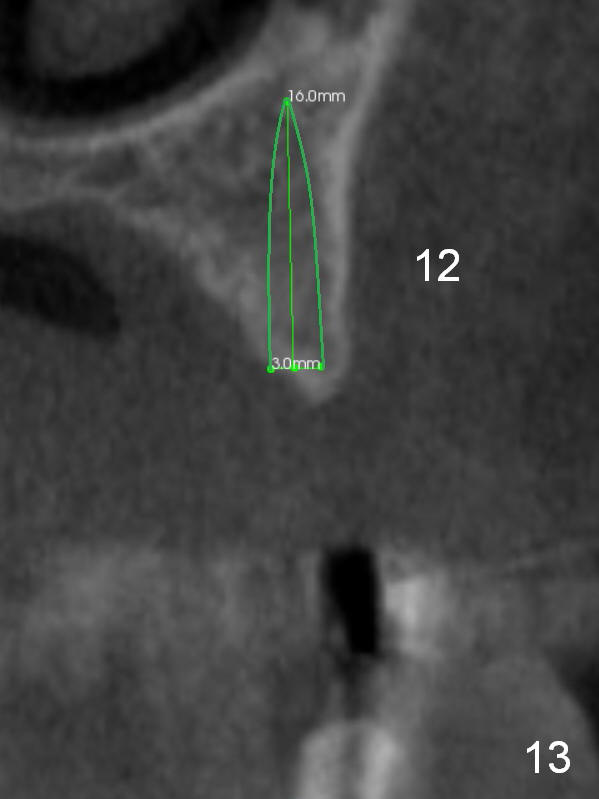
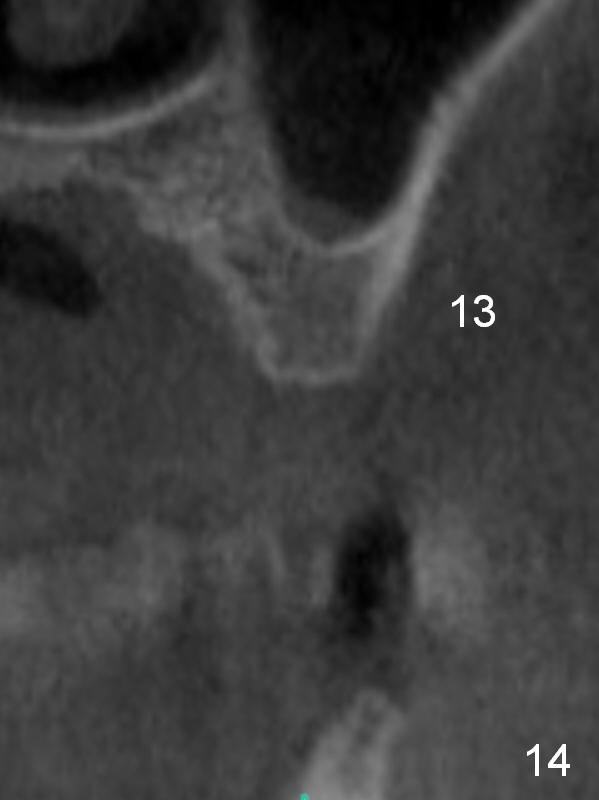
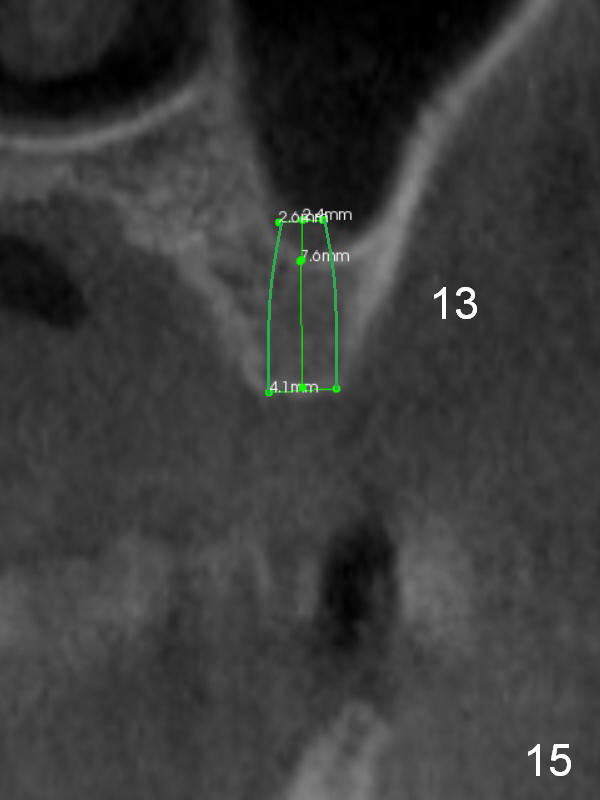
The ridge at #12 becomes a little bit wider and a 1-piece implant is placed palatal (Fig.13). The height of the alveolus and low bone density at #13 are limiting factors (Fig.14). The solutions will be sinus lift and bone condensation (Fig.15).
Make initial osteotomy with the smallest drill through a surgical stent before incision. Prepare 2 of 1-piece implant kits and surgical handpiece with the narrowest long-shanked burs. If the suction-down surgical stent is unstable or unreliable, use his upper RPD (to be modified). Draw blood for 4-6 pieces of PRF membrane.
Return to
Lower Arch Reconstruction
1 Piece
Resection
19
IBS
Chinese,
Atrophic Ridge
Xin Wei, DDS, PhD, MS 1st edition 02/04/2016, last revision 08/05/2018