


|
|
|
|
|
|
|
|
|
|
|
Drawback of Over-expansion
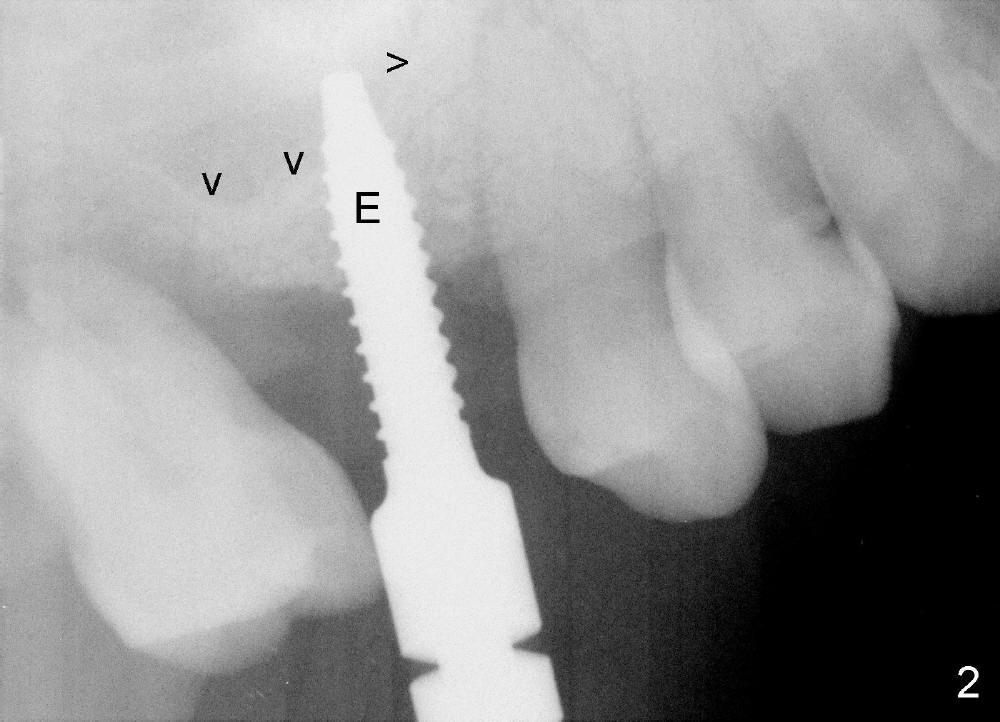
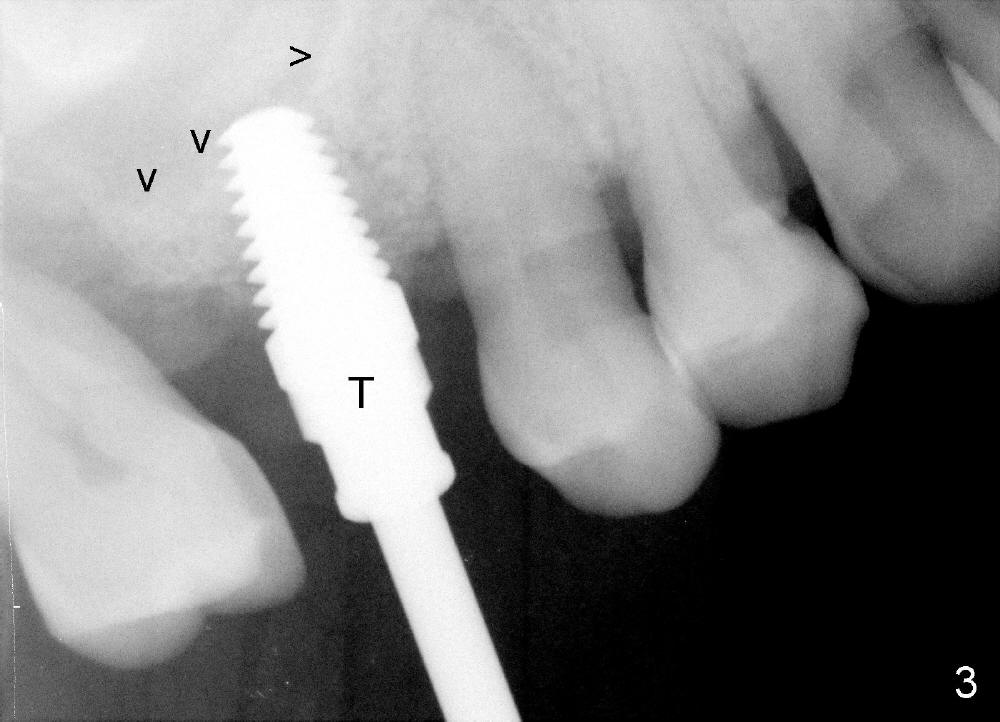
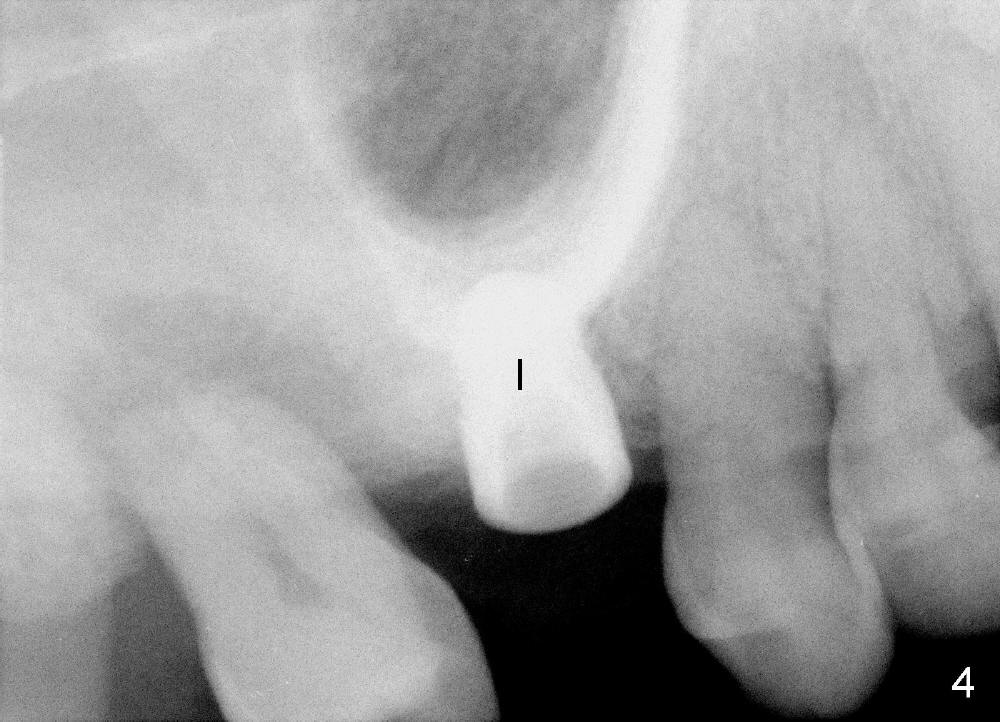
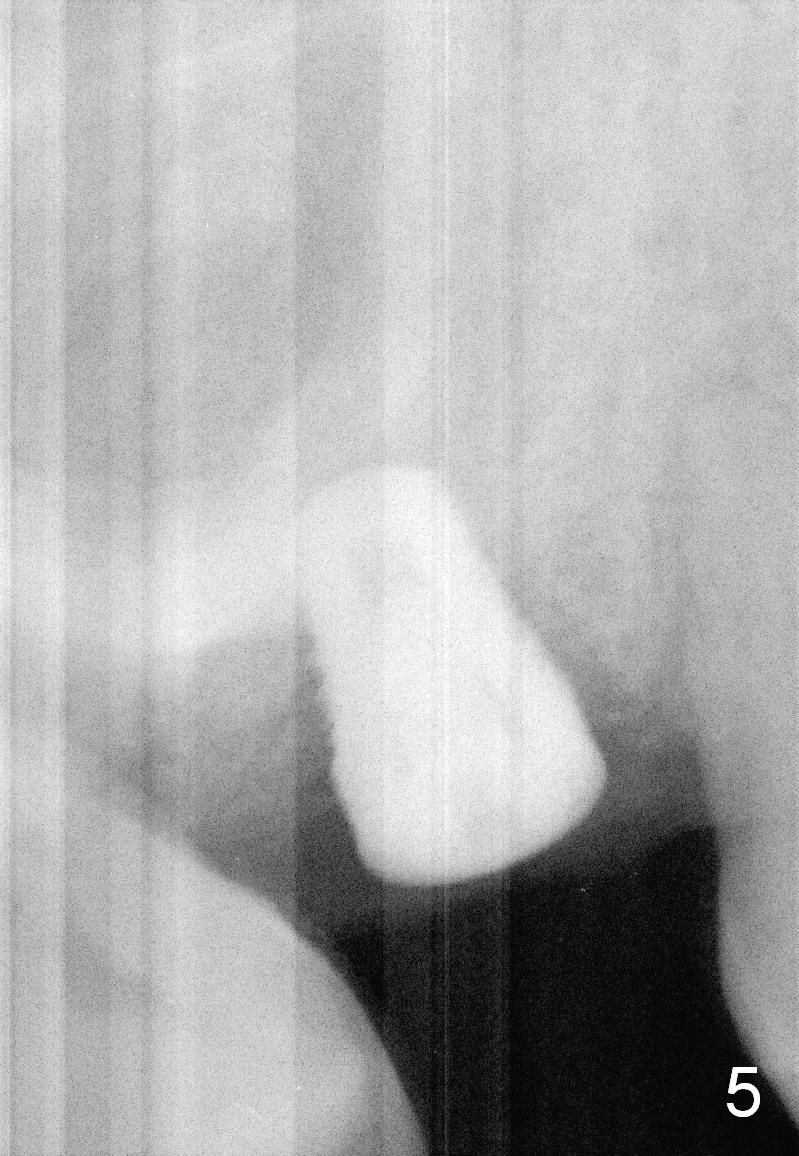
Bone expander kit is planned for for the case at the site of #3 with apparently normal buccolingual width (Fig.1). Bone density proves to be not low intraoperatively. First, when the 1.6 mm pilot drill is being used, the bone does not feel soft. Second, the first expander (2.6 mm, Fig.2 E) cannot be driven into the osteotomy (following the pilot drill) unless 2.5 mm reamer is used. Third, when larger expanders (until 3.8 mm) and 5x11 mm tap (Fig.3 T) are being used, the distobuccal plate starts to crack, although insertion torque of 5.3x8 mm implant is >50 Ncm (Fig.4). Using bone expanders is time consuming. In brief, when the buccolingual width is within normal limit and bone density is not low, traditional osteotomy should be adopted. It is better to use reamers to collect autogentous bone at the same time. The bone can be put back later into the osteotomy for sinus lift. Another drawback of this case is that the implant is not placed deep enough (Fig.5: 3 months postop). When a crown is cemented 1 year 4 months postop, the distal coronal portion of the implant is supragingival, although there is no infection.
Although the tooth #2 (Fig.4) needs extraction and immediate implant next time, the patient has lost #8 and 9 for long time. The bone also looks dense. Are we going to use bone expansion technique?
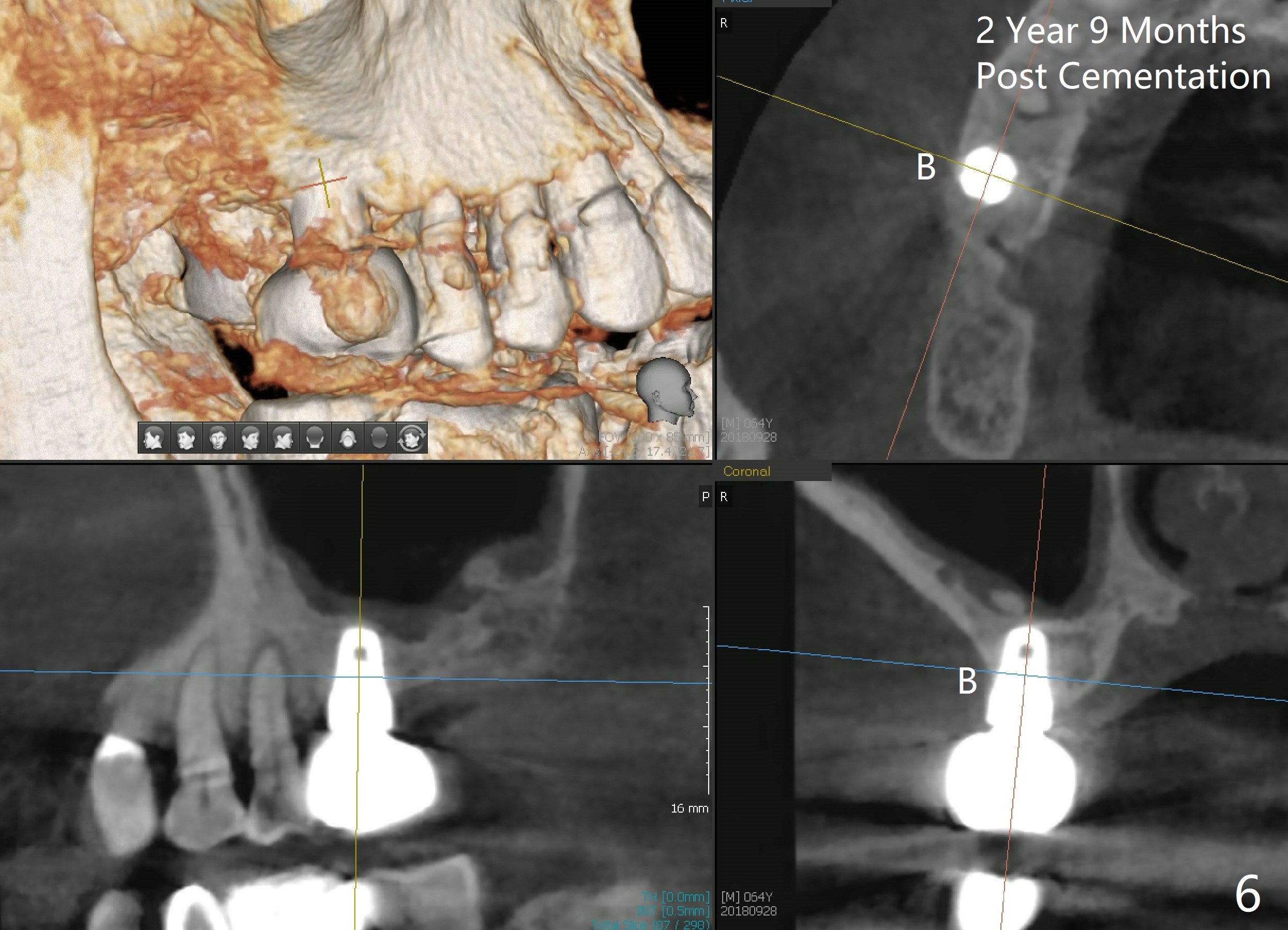
The implant is also found to have been placed buccal (Fig.6 B (CBCT 2 years 9 months post cementation)). In spite of one buccal thread exposure (Fig.8 I), there is no sign of periimplantitis 5 years 3 months post cementation, as related to good oral hygiene (Fig.7).
Return to Sinus Lift, Instrument, Professionals 8/9 10 14 15 19 30 12 第二磨牙即种 4
Xin Wei, DDS, PhD, MS 1st edition 08/12/2014, last revision 05/06/2021