




|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
||
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||
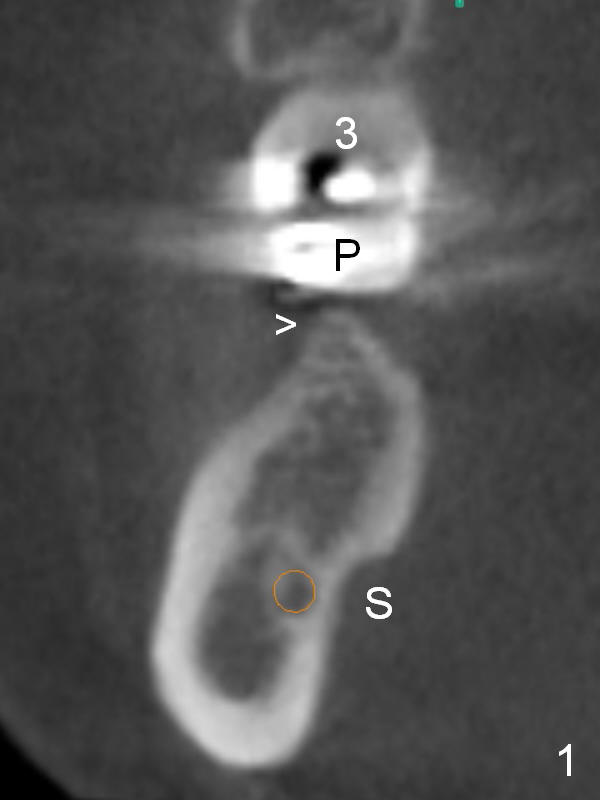
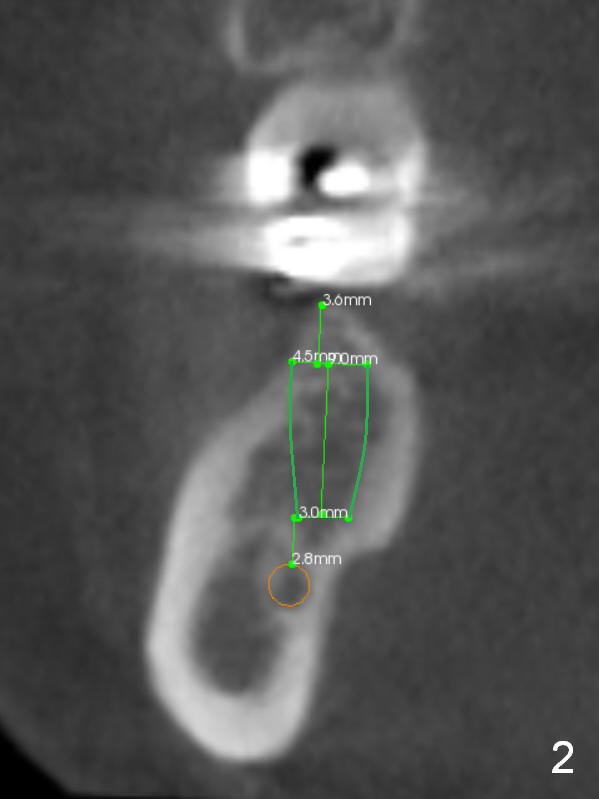
Pointed Ridge
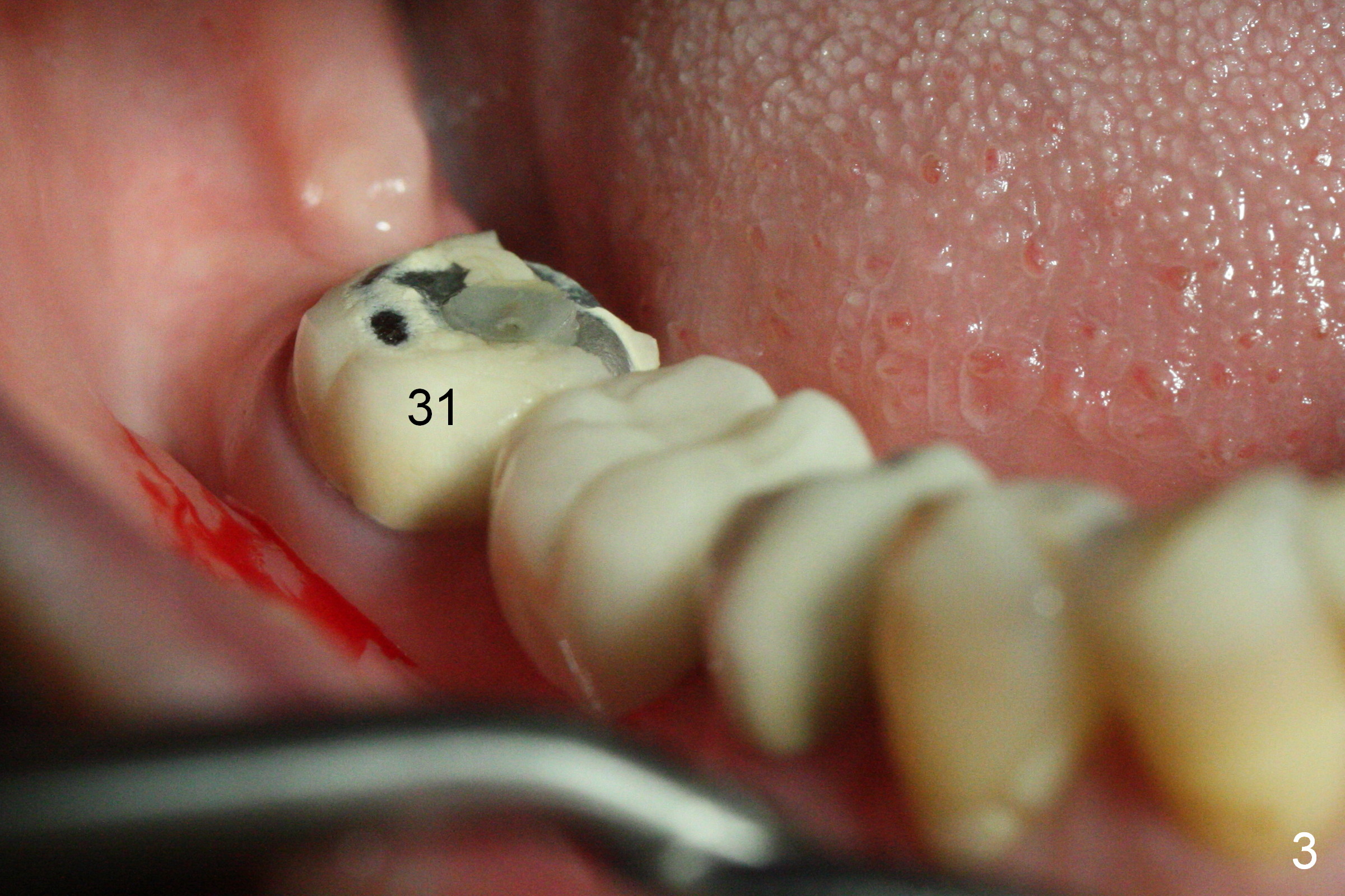
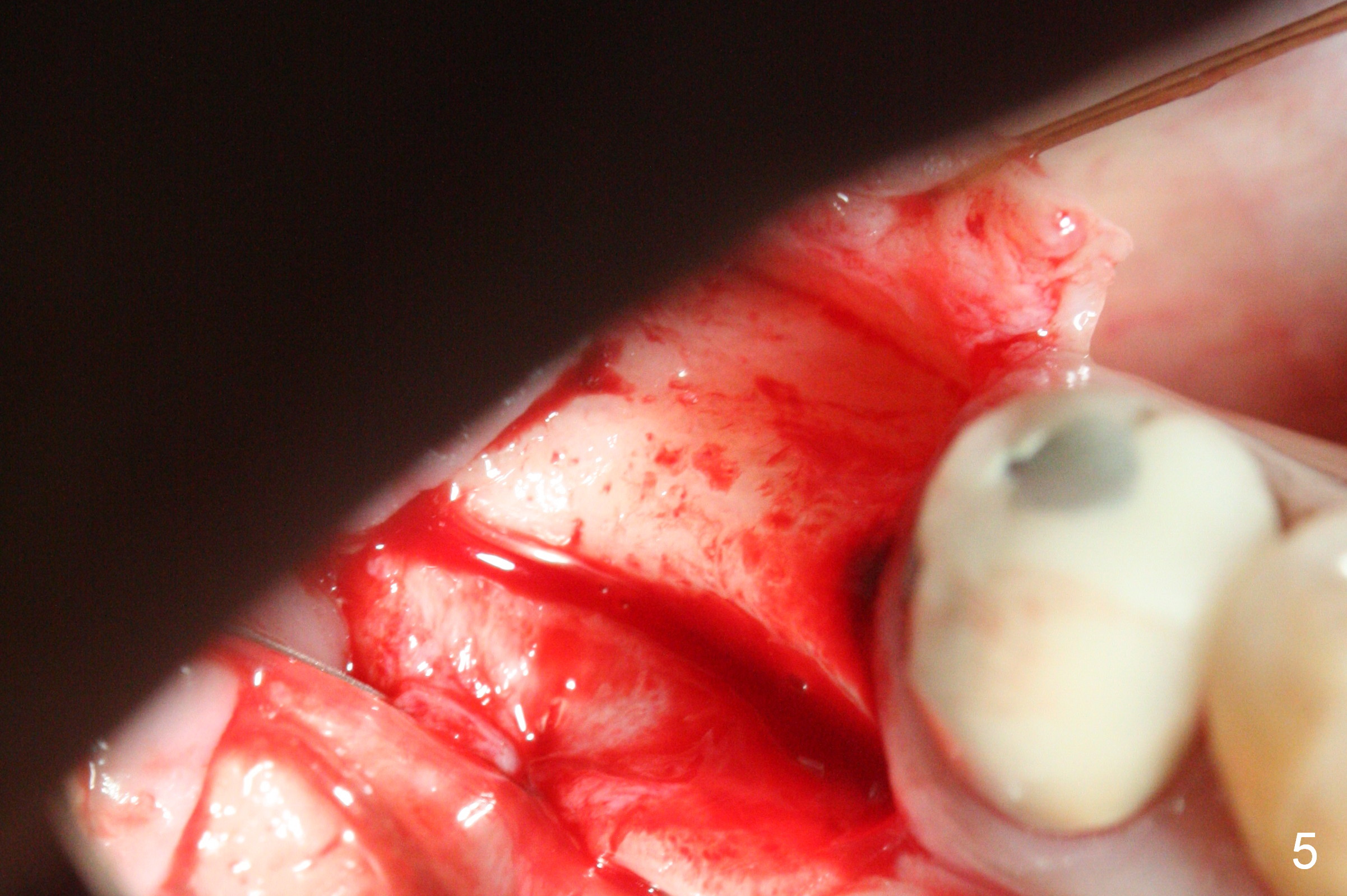
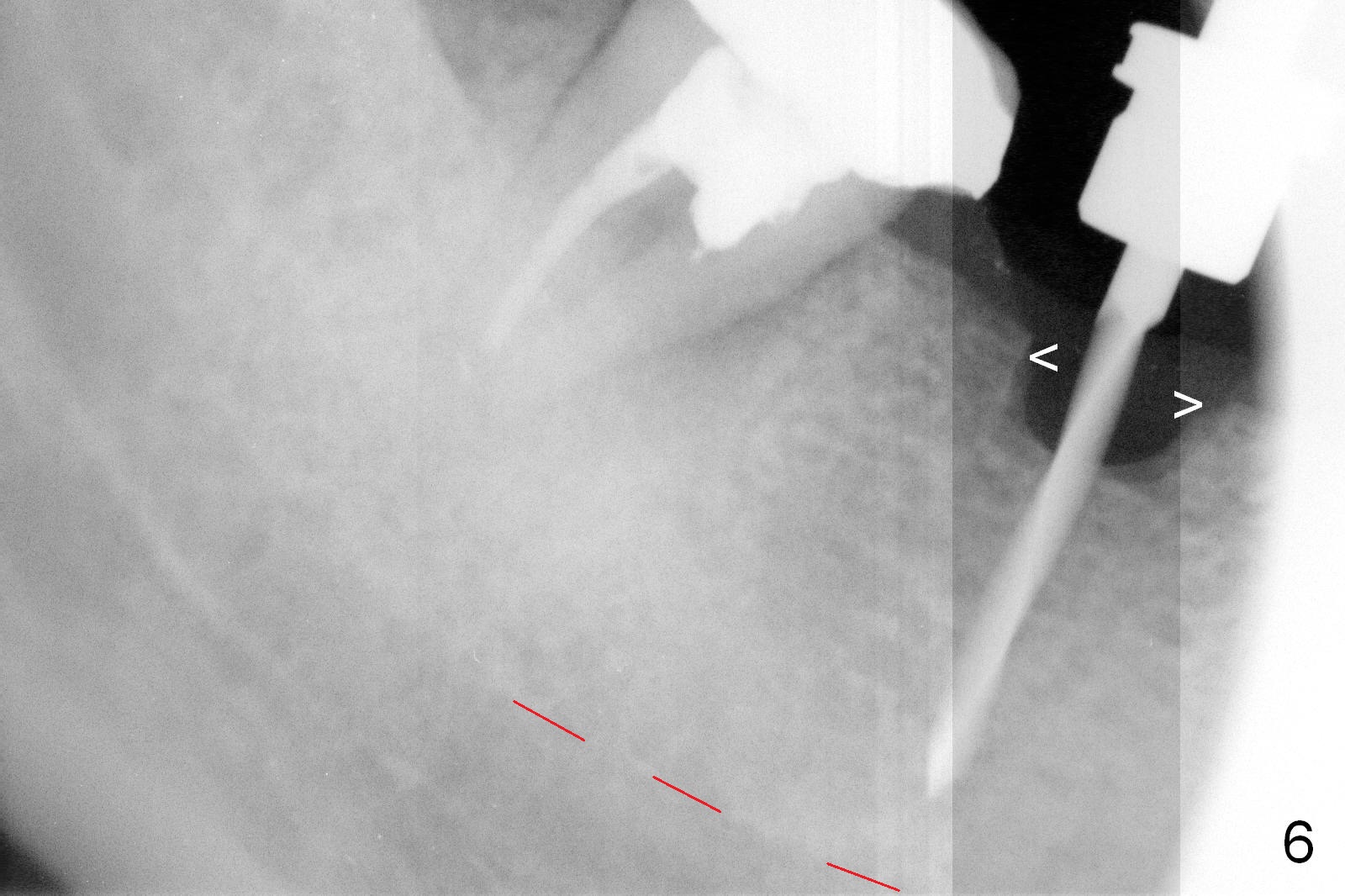
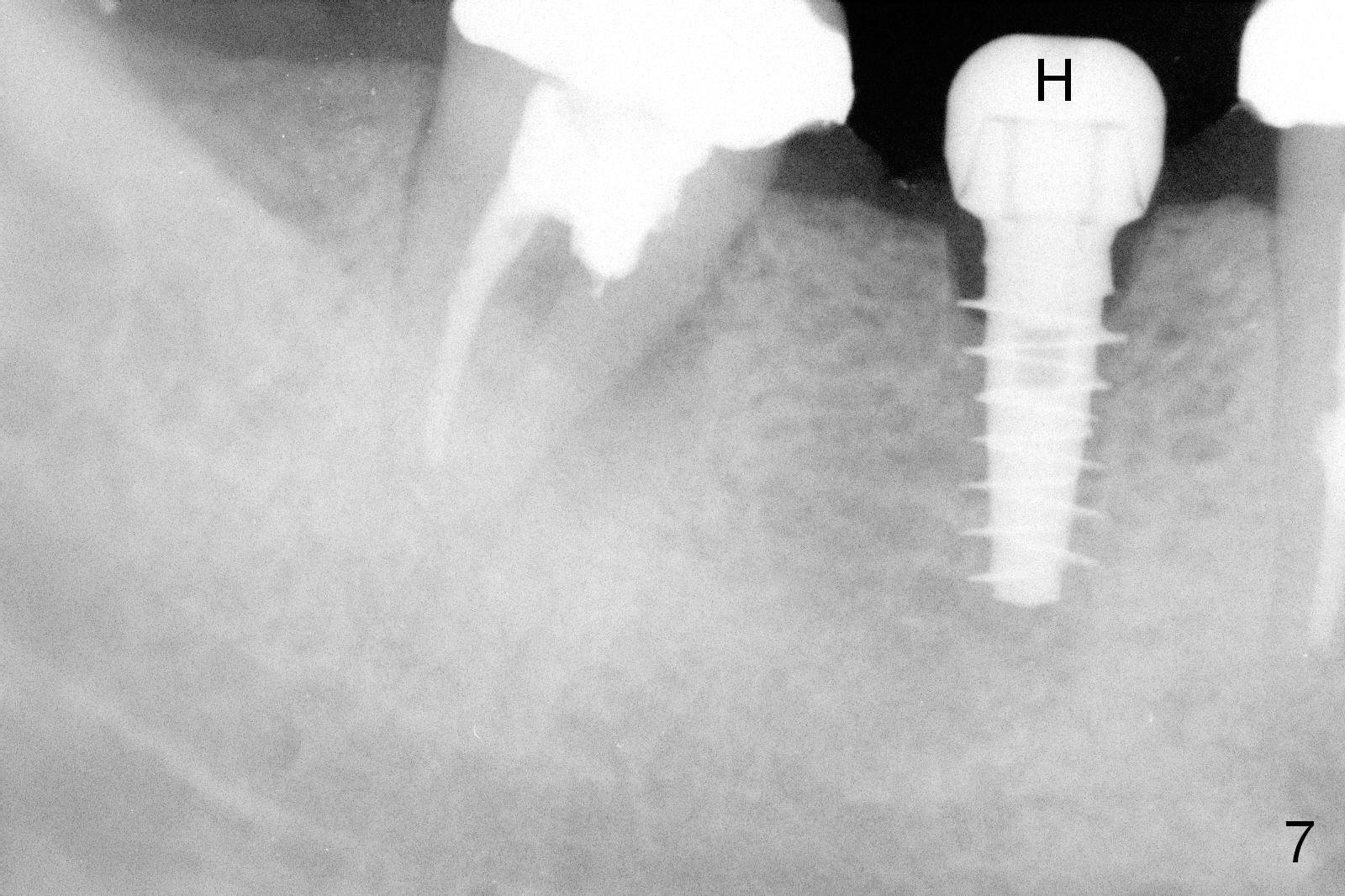
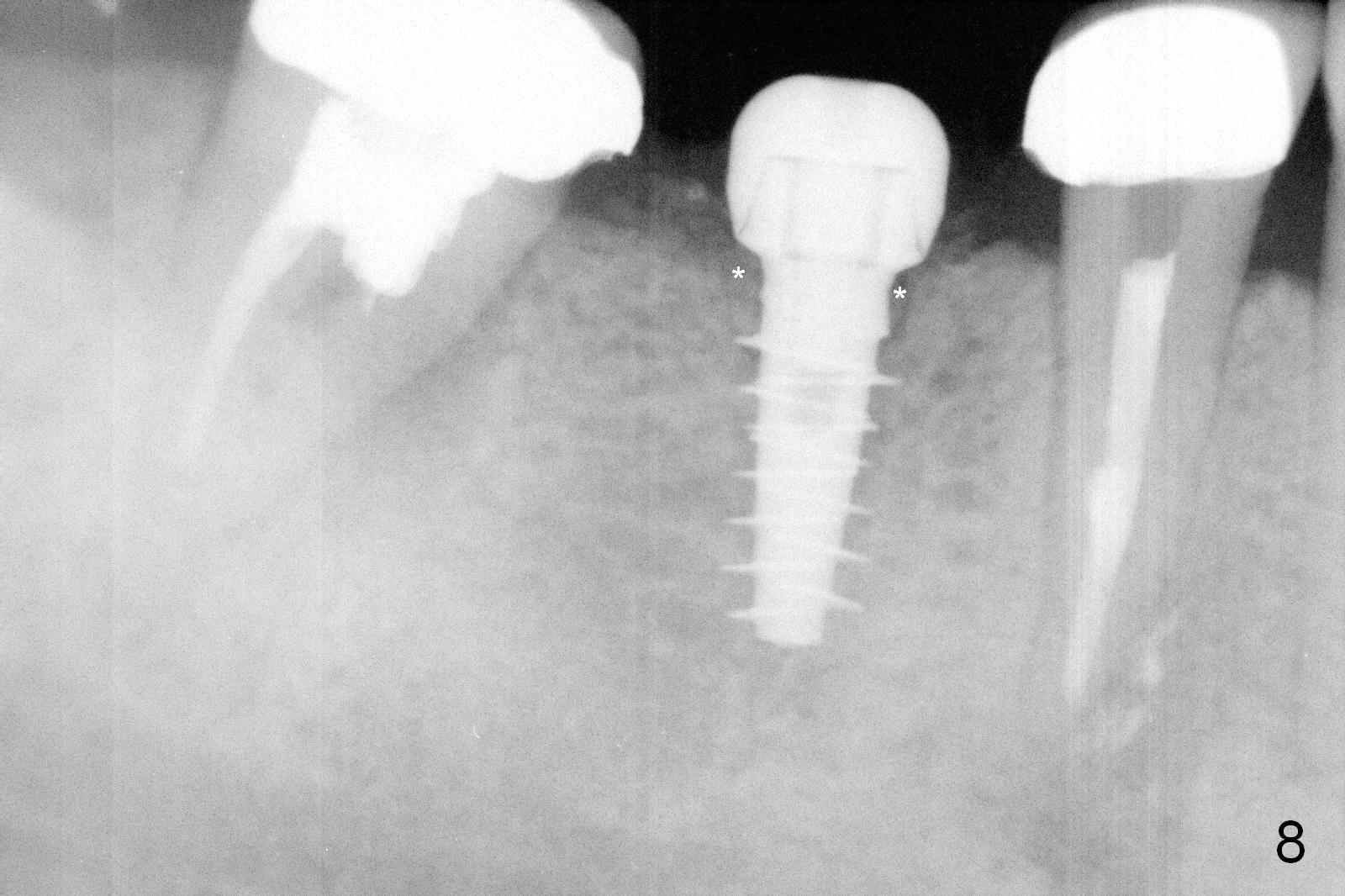
CBCT was taken (Fig.1,2 (P: pontic; S; submandibular fossa)) several months prior to #29 and 31 RCT and #31 porcelain chip (Fig.3). When the bridge is sectioned, the pointed ridge at #30 (Fig.1) is confirmed (Fig.4,5). After flattening the ridge until 6 mm buccolingually (Fig.6 arrowheads), osteotomy is initiated with 1.6 mm drill at 9 mm; there is 2.5 mm clearance from the superior border of the Inferior Alveolar Canal (red dashed line). A 4.5x9(1) mm Magicore is placed with 35 Ncm (insertion torque) after 4.3 mm Magic Drill; a 4.5 mm healing abutment (Fig.7 H). An error occurs because of using 1 mm cuff of the Magicore. Ideally 3 or 4 mm cuff should have been used because of reduction of the ridge by ~ 3 mm (Fig.2). The result of the error is failure of placing the implant at the desirable depth (<9 mm). The coronal threads are exposed and have to be covered by bone graft (autogenous bone and allograft (.5-1.5 mm) (Fig.8 *), followed by collagen dressing. Extra suturing is done to securely close the wound (Fig.9), followed by periodontal dressing (data not shown).
The wound is healing 8 days postop (Fig.10). Because of the short cuff (subgingival margin), screw retention type of restoration will be used, in contrast to cement type of the 2nd case. In fact, FC one is used.
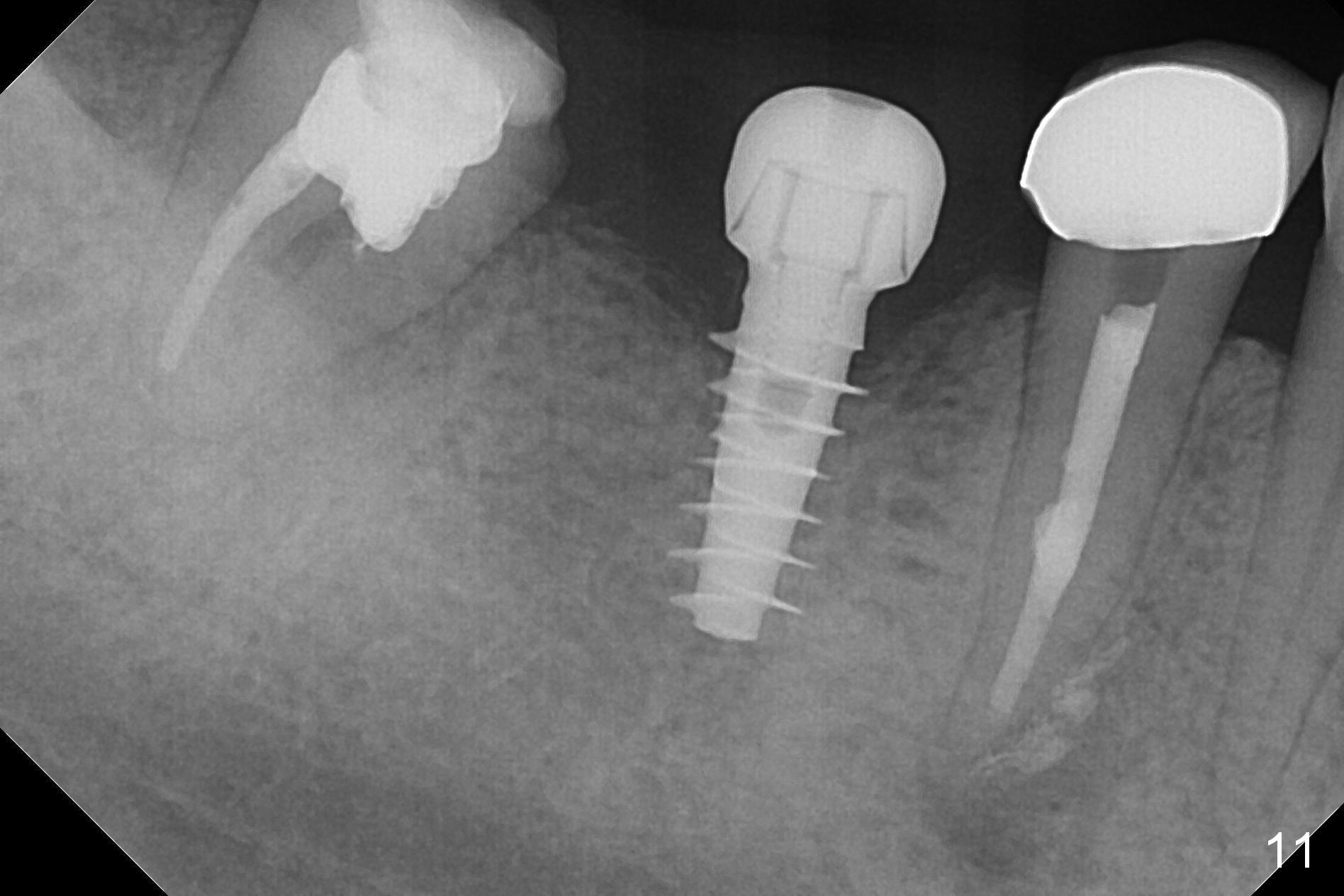
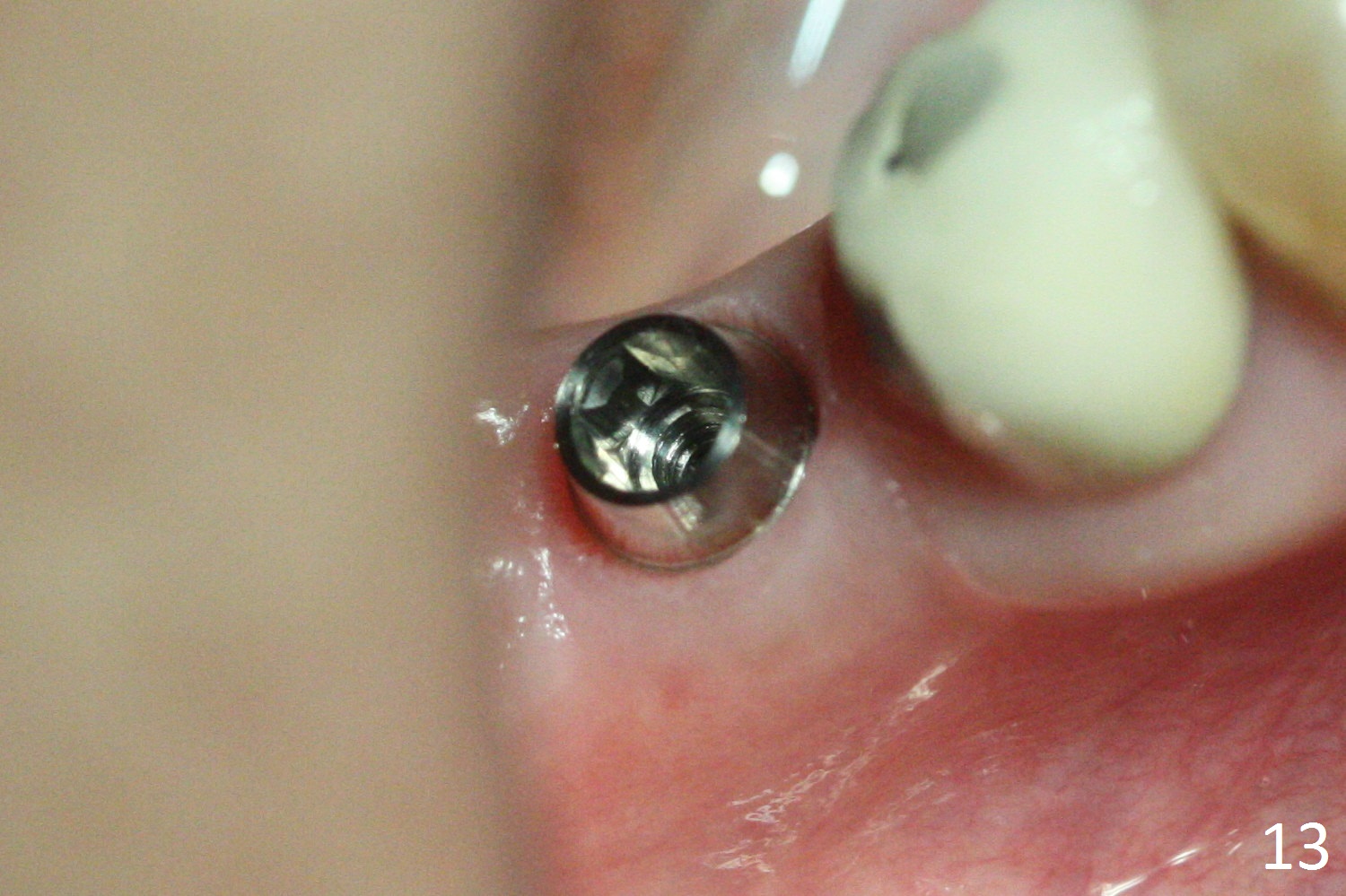
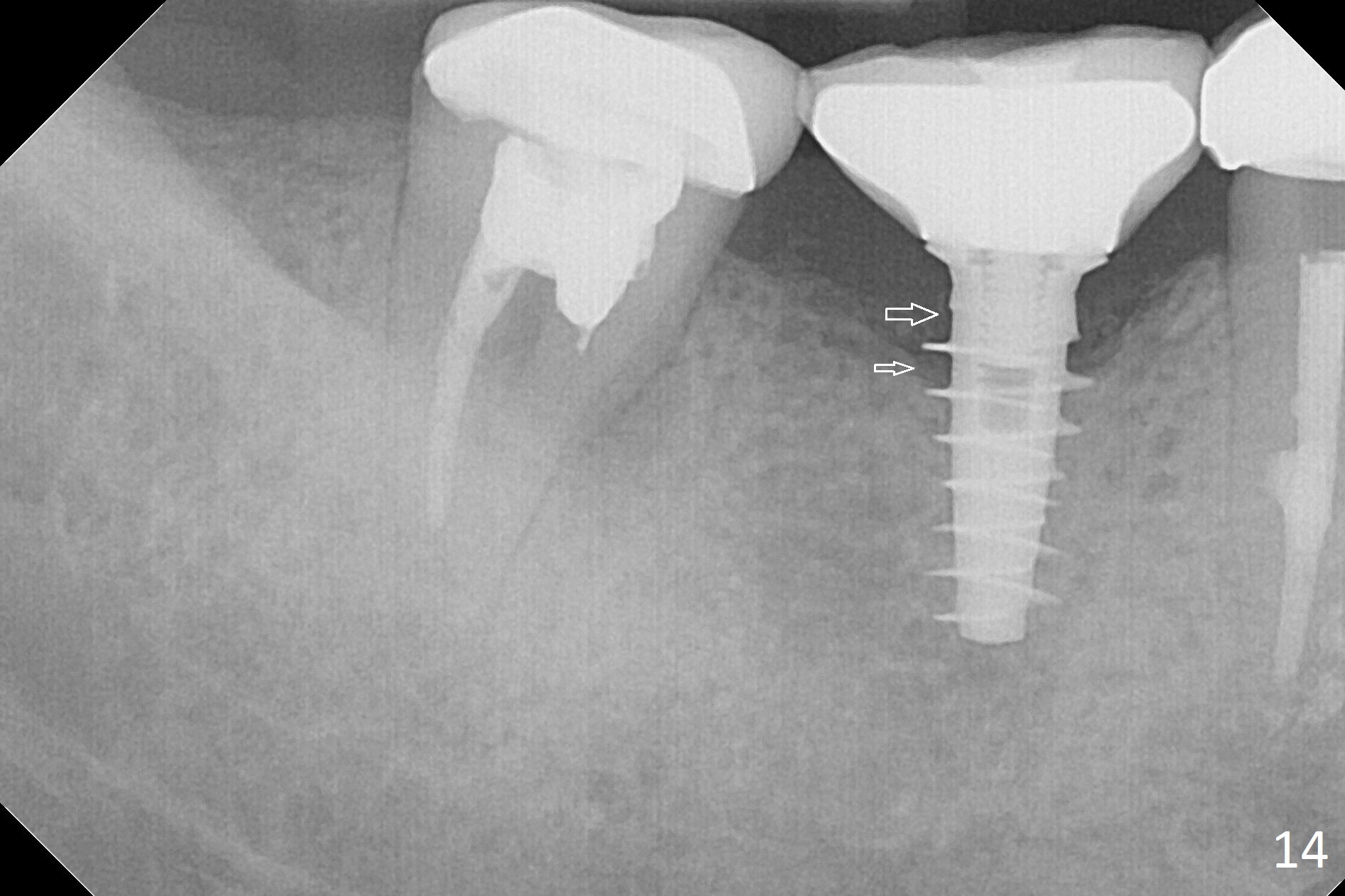
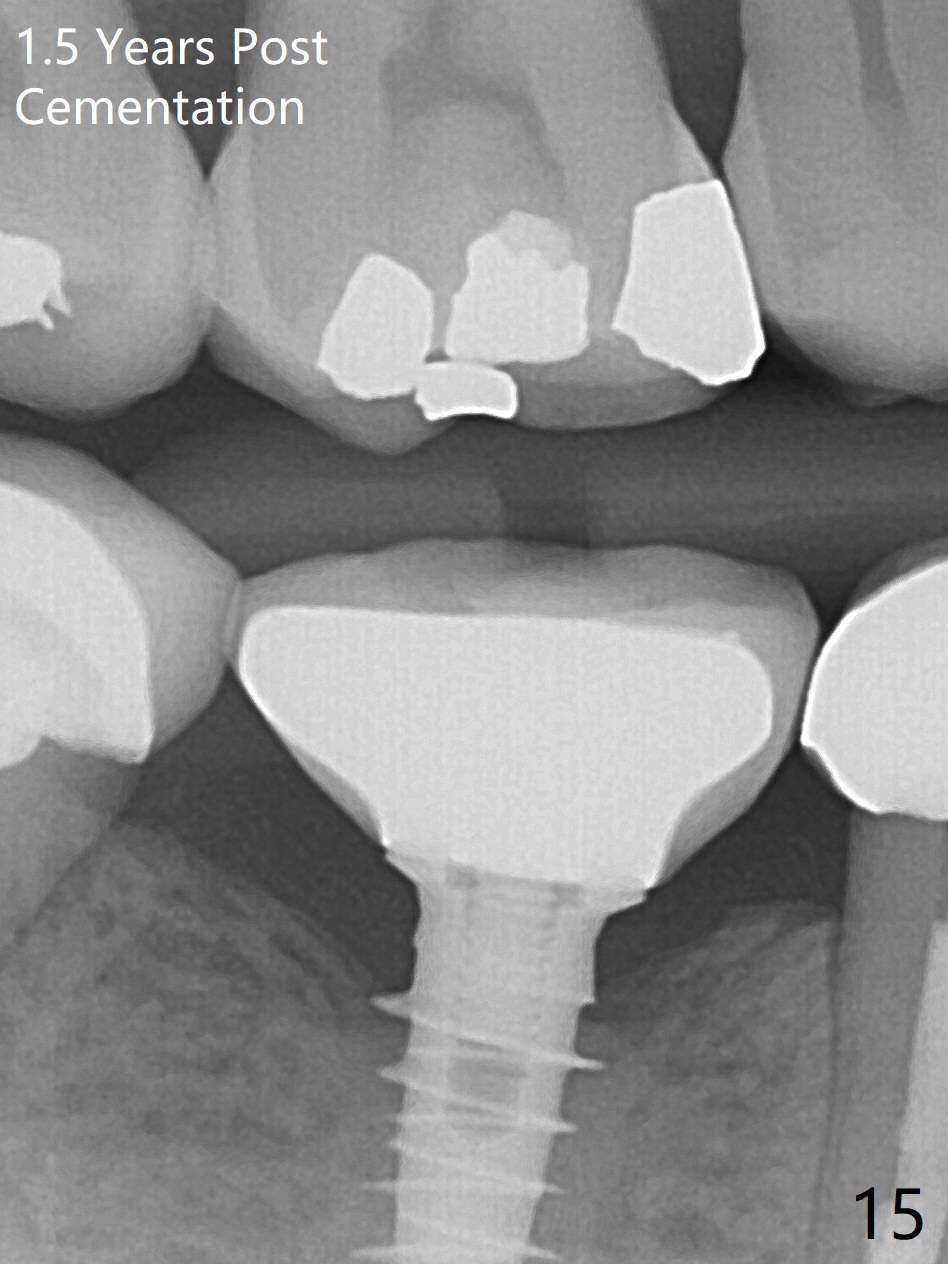
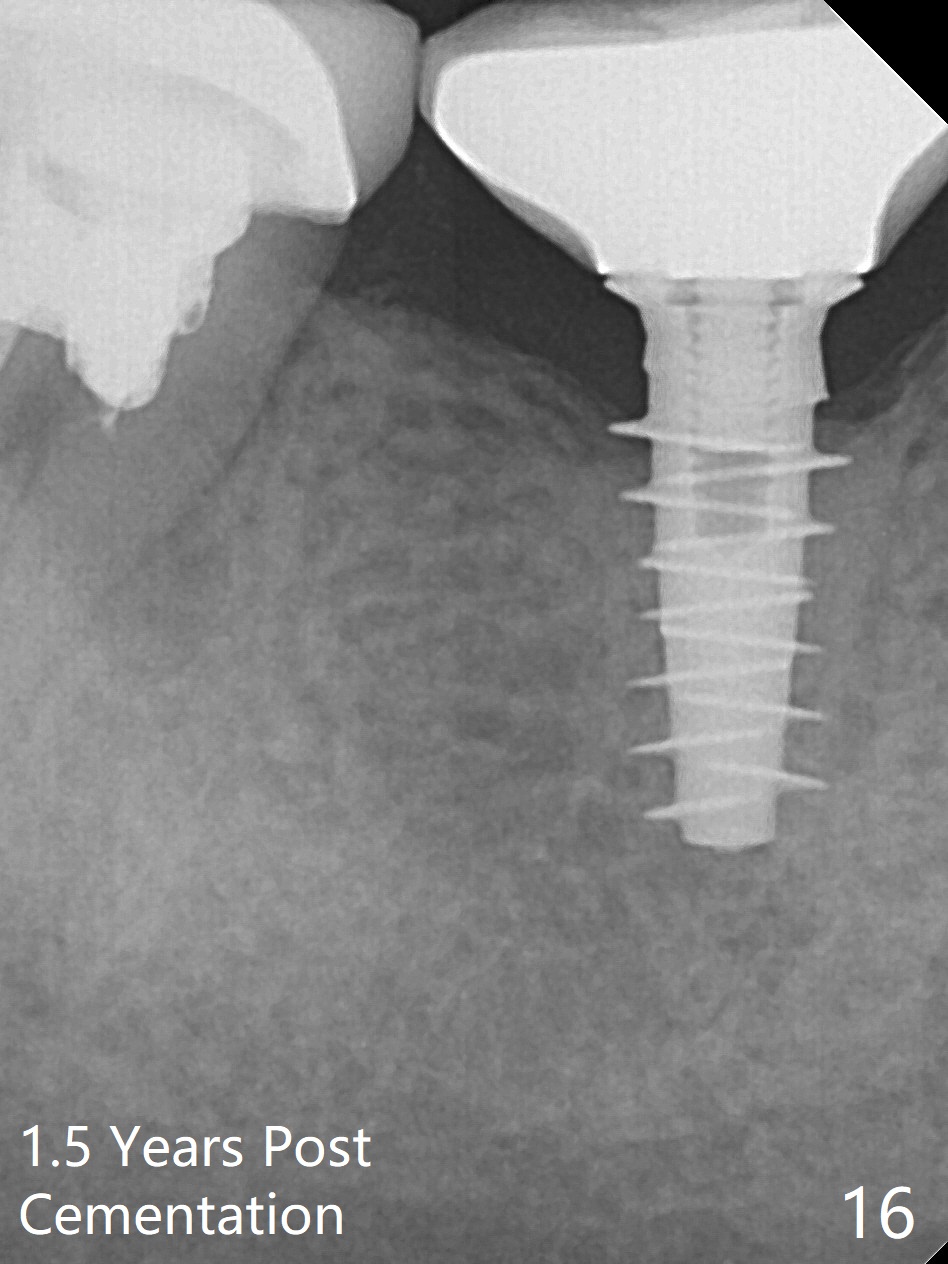
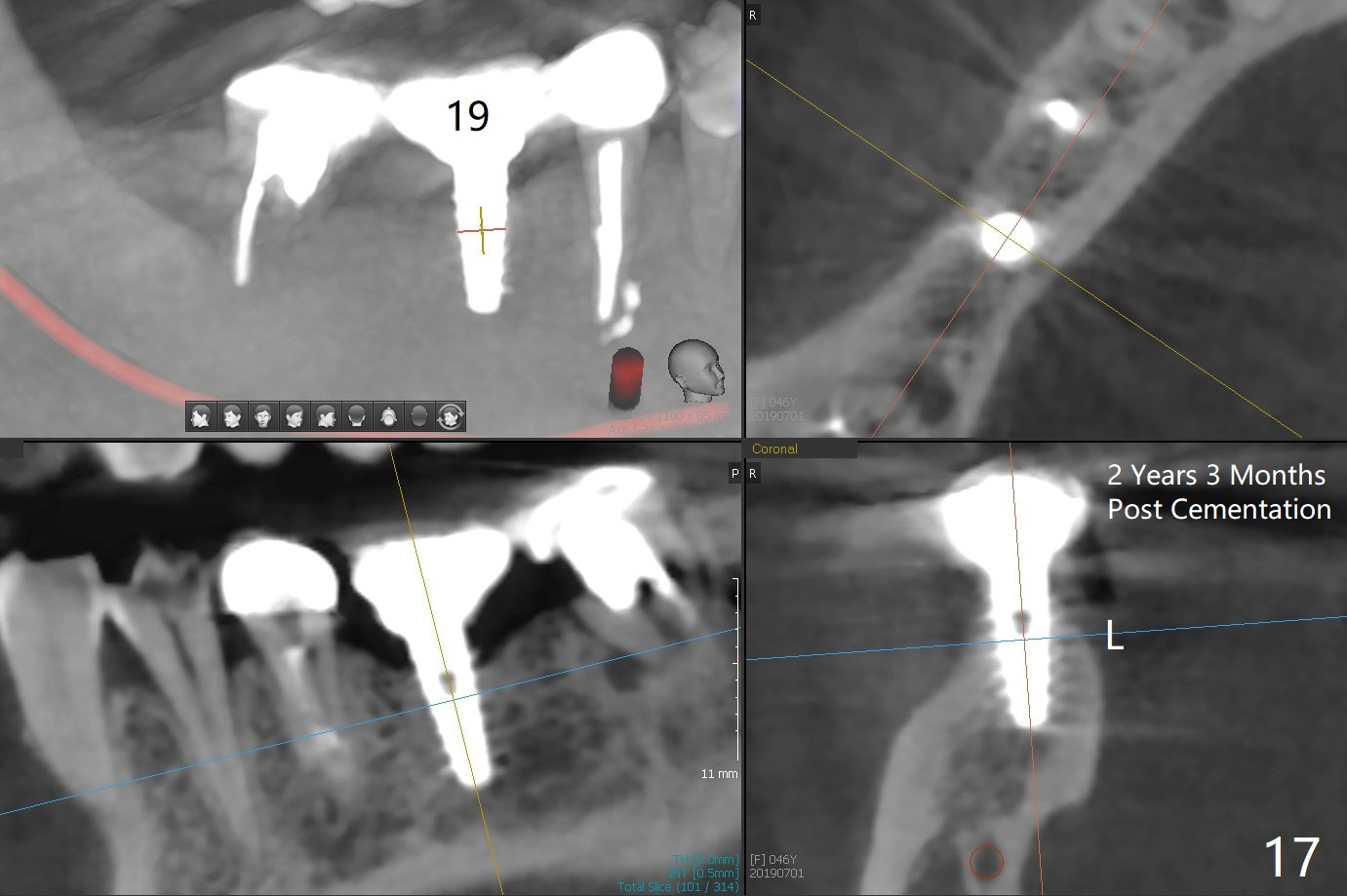
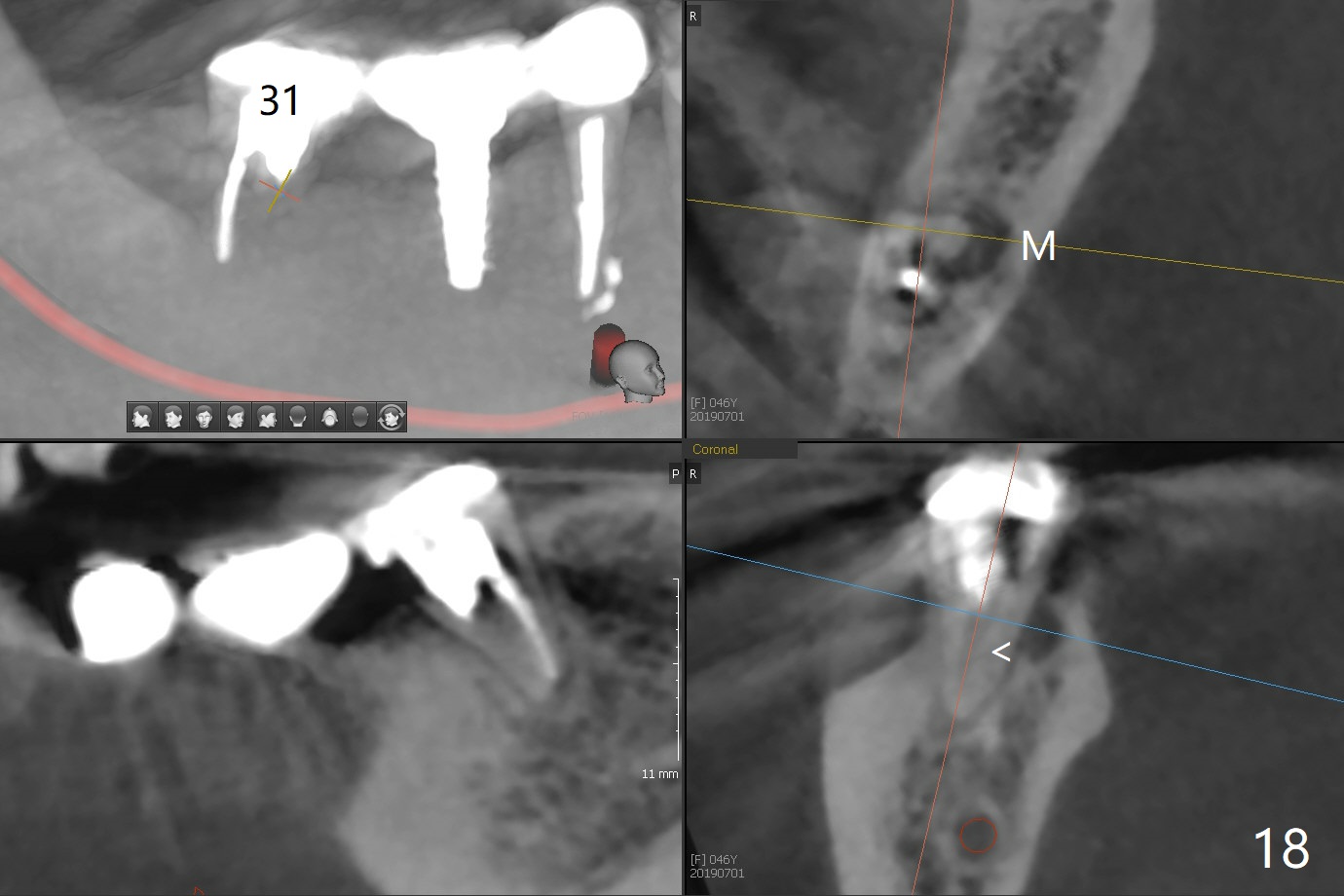
Splinted provisional is fabricated #30 and 31 one month postop. The patient returns for final restoration (single units) nearly 4 months postop (Fig.11). Since the margin is subgingival, a screw type crown is fabricated for #30 (Fig.12). The buccal gingiva looks convex after healing cap removal (Fig.13, as compared to Fig.4 (concave)). PA is taken immediately post tightening and cementation (Fig.14, 5 months postop). It appears that new bone has grown between the most coronal threads (arrows). The bone density immediately around the implant appears to increase 1.5 years post cementation (Fig.15,16). She returns because of failure of 18-20 bridge (implants will be placed at 18/19). The implant at #30 is in fact not placed deep enough; the coronal threads seem to be exposed, although there is no periimplantitis (Fig.17 CT). The tooth #31 is symptomatic; the mesial canal is missing (Fig.18 M, <). The gingiva around the crowns at #30 and 31 remains healthy 2 years 4 months post cementation (Fig.19). Metal exposure of the crown at #31 is intentional. Occlusal reduction is done to alleviate periapical re-infection (Fig.18).
Return to
Lower
Molar Immediate Implant,
IBS,
Dr.
Wang's Response, Implant & Ortho
2,
Magicore Cases
Xin Wei, DDS, PhD, MS 1st edition 11/01/2016, last revision 08/07/2019